

Implementation of systematic safety checklists in a neurocritical care unit: a quality improvement study
- PMID: 36588320
- PMCID: PMC9743379
- DOI: 10.1136/bmjoq-2022-001824
Implementation of systematic safety checklists in a neurocritical care unit: a quality improvement study
Abstract
Background and objectives: Structured and systematised checklists have been shown to prevent complications and improve patient care. We evaluated the implementation of systematic safety checklists in our neurocritical care unit (NCCU) and assessed its effect on patient outcomes.
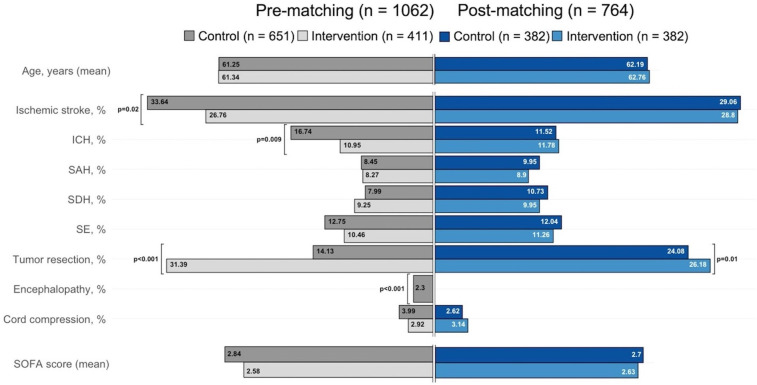
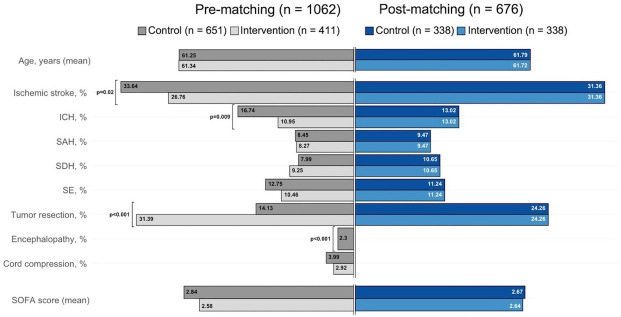
Design/methods: This quality improvement project followed a Plan-Do-Study-Act (PDSA) methodology. A checklist for medication reconciliation, thromboembolic prophylaxis, glycaemic control, daily spontaneous awakening, breathing trial, diet, catheter/lines duration monitoring and antibiotics de-escalation was implemented during daily patient rounds. Main outcomes included the rate of new infections, mortality and NCCU-length of stay (LOS). Intervened patients were compared with historical controls after propensity score and Euclidean distance matching to balance baseline covariates.
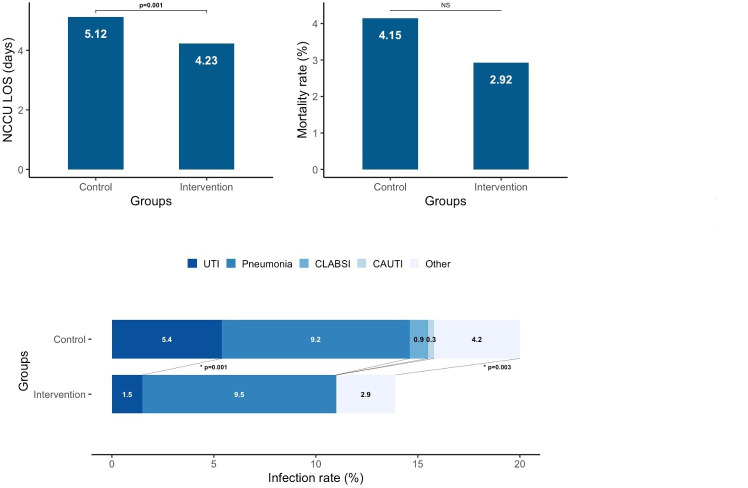
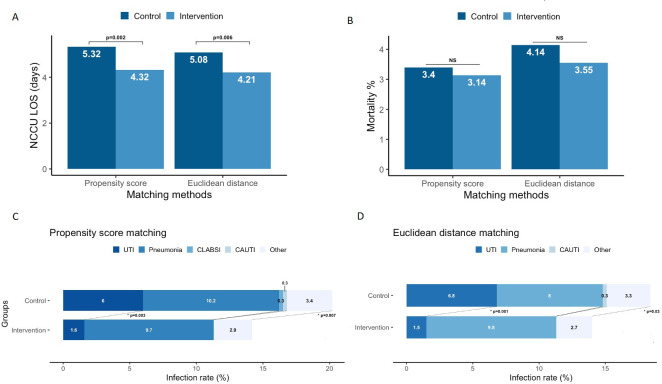
Results: After several PDSA iterations, we applied checklists to 411 patients; the overall average age was 61.34 (17.39). The main reason for admission included tumour resection (31.39%), ischaemic stroke (26.76%) and intracerebral haemorrhage (10.95%); the mean Sequential Organ Failure Assessment (SOFA) score was 2.58 (2.68). At the end of the study, the checklist compliance rate throughout the full NCCU stays reached 97.11%. After controlling for SOFA score, age, sex and primary admitting diagnosis, the implementation of systematic checklists significantly correlated with a reduced LOS (ß=-0.15, 95% CI -0.24 to -0.06), reduced rate of any new infections (OR 0.59, 95% CI 0.40 to 0.87) and reduced urinary tract infections (UTIs) (OR 0.23, 95% CI 0.09 to 0.55). Propensity score and Euclidean distance matching yielded 382 and 338 pairs with excellent covariate balance. After matching, outcomes remained significant.
Discussion: The implementation of safety checklists in the NCCU proved feasible, easy to incorporate into the NCCU workflow, and a helpful tool to improve adherence to practice guidelines and quality of care measurements. Furthermore, our intervention resulted in a reduced NCCU-LOS, rate of new infections and rate of UTIs compared with propensity score and Euclidean distance matched historical controls.
Keywords: checklists; critical care; health services research; quality improvement.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Effect of a Quality Improvement Intervention With Daily Round Checklists, Goal Setting, and Clinician Prompting on Mortality of Critically Ill Patients: A Randomized Clinical Trial.JAMA. 2016 Apr 12;315(14):1480-90. doi: 10.1001/jama.2016.3463. JAMA. 2016. PMID: 27115264 Clinical Trial.
-
Health Care-Associated Infections in a Neurocritical Care Unit of a Developing Country.Neurocrit Care. 2020 Jun;32(3):836-846. doi: 10.1007/s12028-019-00856-8. Neurocrit Care. 2020. PMID: 31562598
-
Do Digital Handover Checklists Influence the Clinical Outcome Parameters of Intensive Care Unit Patients? A Randomized Controlled Pilot Study.Front Med (Lausanne). 2021 Apr 20;8:661343. doi: 10.3389/fmed.2021.661343. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33959627 Free PMC article.
-
Prospective application of the interdisciplinary bedside rounding checklist 'TEMP' is associated with reduced infections and length of hospital stay.BMJ Open Qual. 2022 Dec;11(4):e002045. doi: 10.1136/bmjoq-2022-002045. BMJ Open Qual. 2022. PMID: 36588303 Free PMC article. Review.
-
Surgical safety checklists: a review.ANZ J Surg. 2014 Mar;84(3):148-54. doi: 10.1111/ans.12168. Epub 2013 Apr 18. ANZ J Surg. 2014. PMID: 23601094 Review.
Cited by
-
Optimizing ward rounds: systematic review and meta-analysis of interventions to enhance patient safety.Br J Surg. 2025 Mar 28;112(4):znaf041. doi: 10.1093/bjs/znaf041. Br J Surg. 2025. PMID: 40202092 Free PMC article.
-
Impact of Rounding Checklists on the Outcomes of Patients Admitted to ICUs: A Systematic Review and Meta-Analysis.Crit Care Explor. 2024 Aug 20;6(8):e1140. doi: 10.1097/CCE.0000000000001140. eCollection 2024 Aug 1. Crit Care Explor. 2024. PMID: 39162653 Free PMC article.
References
-
- McNett MM, Horowitz DA, Participants in the International Multidisciplinary Consensus Conference on Multimodality Monitoring . International multidisciplinary consensus conference on multimodality monitoring: ICU processes of care. Neurocrit Care 2014;21 Suppl 2:215–28. 10.1007/s12028-014-0020-x - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical