

Cerebral Visual Loss
- PMID: 36589033
- PMCID: PMC9795709
- DOI: 10.4103/aian.aian_136_22
Cerebral Visual Loss
Abstract
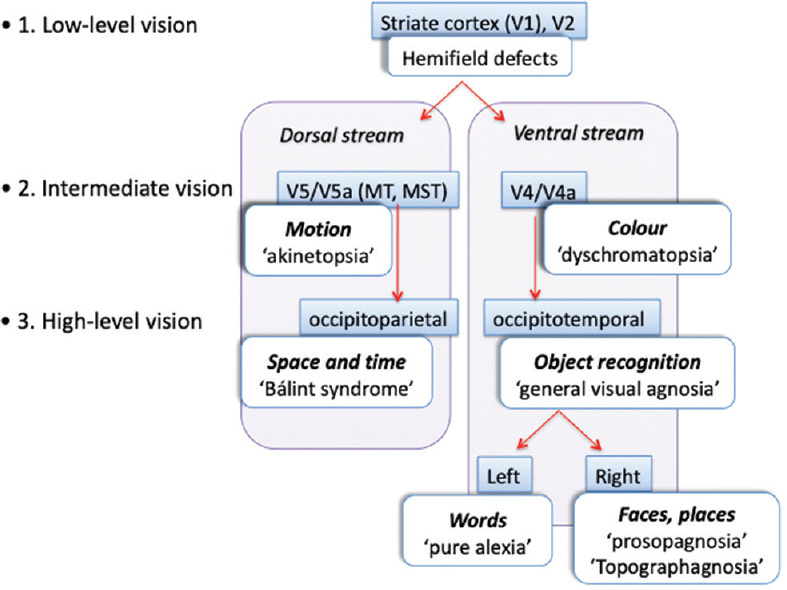
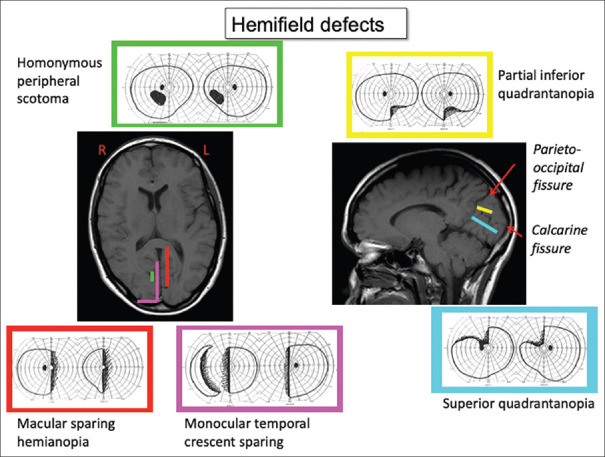
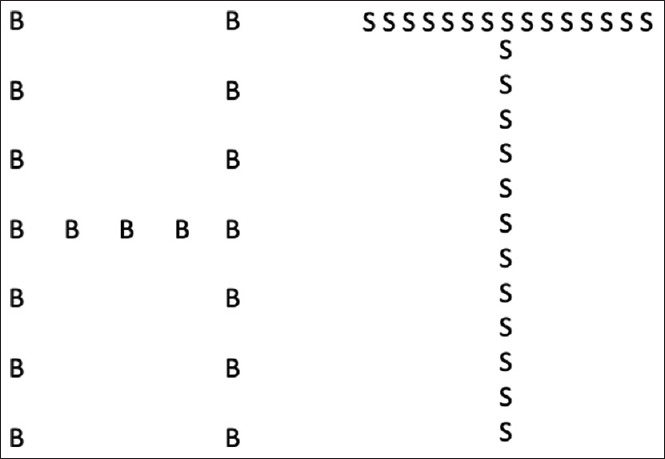
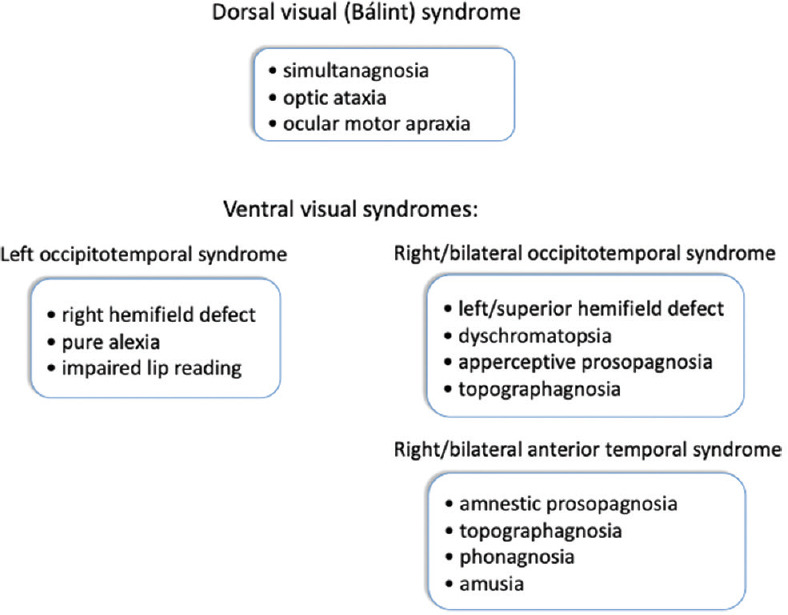
Cerebral visual disorders include a range of common and rare deficits. They can be divided into effects on low-, intermediate-, and high-level forms of visual processing. Low-level deficits are various forms of homonymous hemifield scotomata, which affect all types of vision within their borders. Intermediate-level deficits refer to impairments of colour or motion perception, which affect either one hemifield or the entire field when lesions are bilateral. High-level deficits are divided into those of the ventral (occipitotemporal) or dorsal (occipitoparietal) stream. Occipitotemporal lesions affect various aspects of object recognition, ranging from general visual agnosia to selective agnosias, such as prosopagnosia or topographagnosia from right or bilateral lesions, and pure alexia from left-sided lesions. Occipitoparietal lesions cause the various components of Bálint syndrome, namely, simultanagnosia, optic ataxia, and ocular motor apraxia. They can also cause other impairments of visuospatial or visuotemporal processing, such as astereopsis and sequence-agnosia. Because of anatomic proximity, certain deficits cluster together to form a number of cerebral visual syndromes. Treatment of these disorders remains challenging, with frequent reliance on strategic substitutions rather than restorative approaches.
Keywords: Agnosia; balint; hemianopia.
Copyright: © 2022 Annals of Indian Academy of Neurology.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Shahinfar S, Johnson LN, Madsen RW. Confrontation visual field loss as a function of decibel sensitivity loss on automated static perimetry. Implications on the accuracy of confrontation visual field testing. Ophthalmology. 1995;102:872–7. - PubMed
-
- Zeki SM. A century of cerebral achromatopsia. Brain. 1990;113:1721–77. - PubMed
-
- Bouvier SE, Engel SA. Behavioral deficits and cortical damage loci in cerebral achromatopsia. Cereb Cortex. 2006;16:183–91. - PubMed
