

Uncommon Tumors and Uncommon Presentations of Cancer in the Breast
- PMID: 36589040
- PMCID: PMC9798716
- DOI: 10.1007/s12609-021-00435-x
Uncommon Tumors and Uncommon Presentations of Cancer in the Breast
Abstract
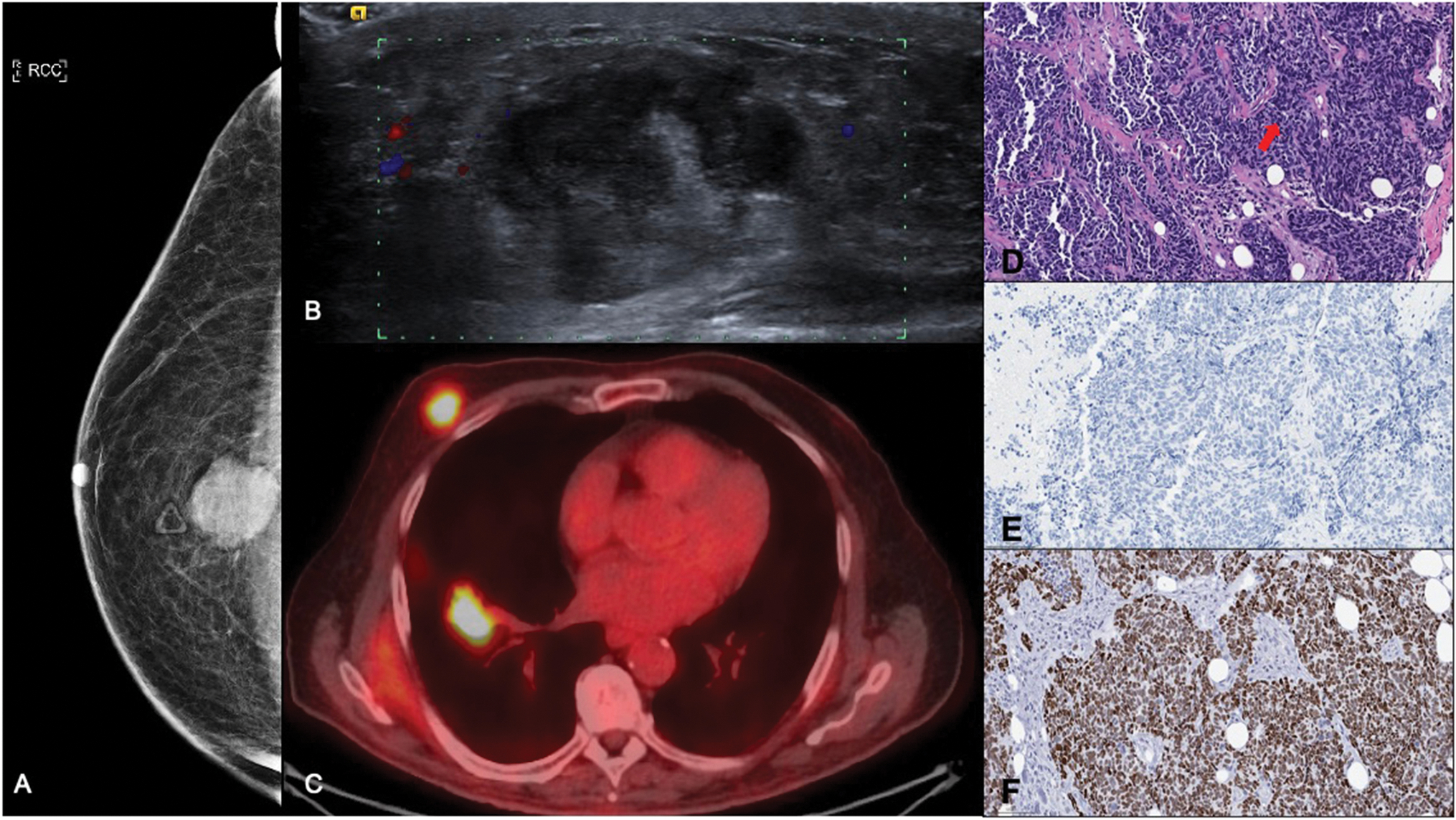
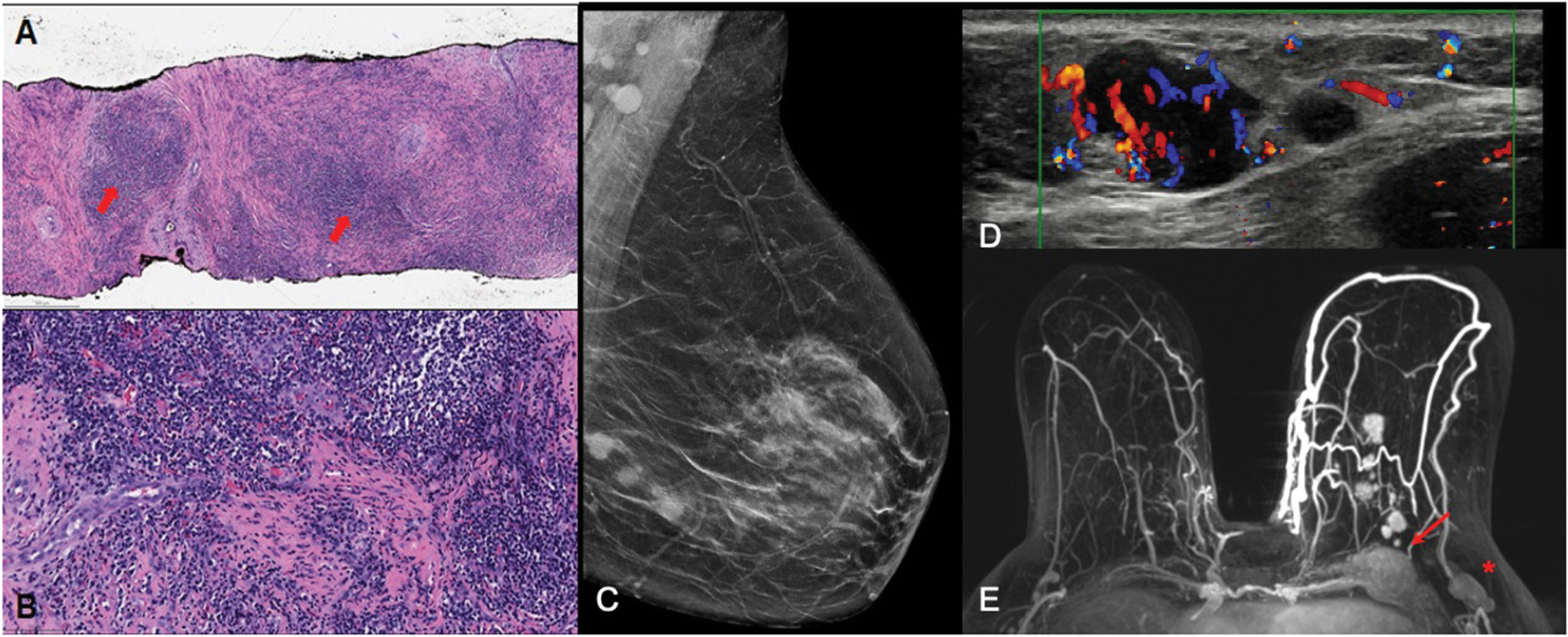
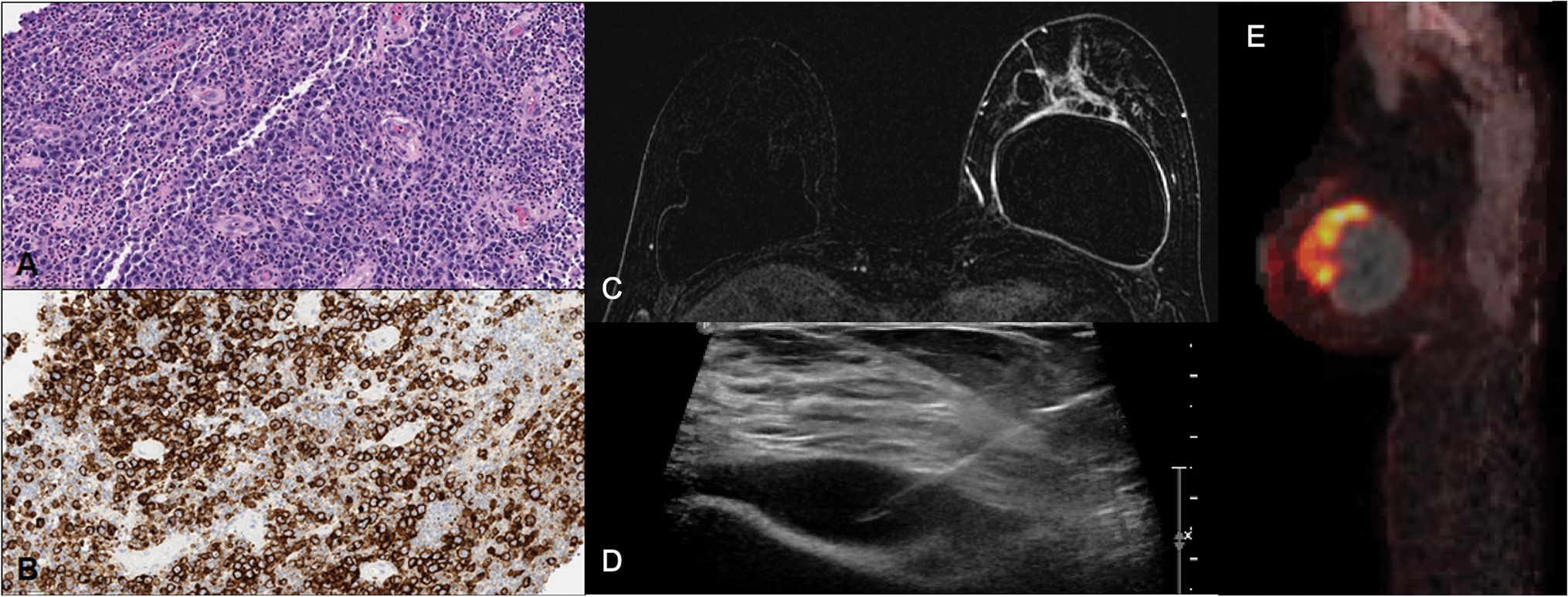
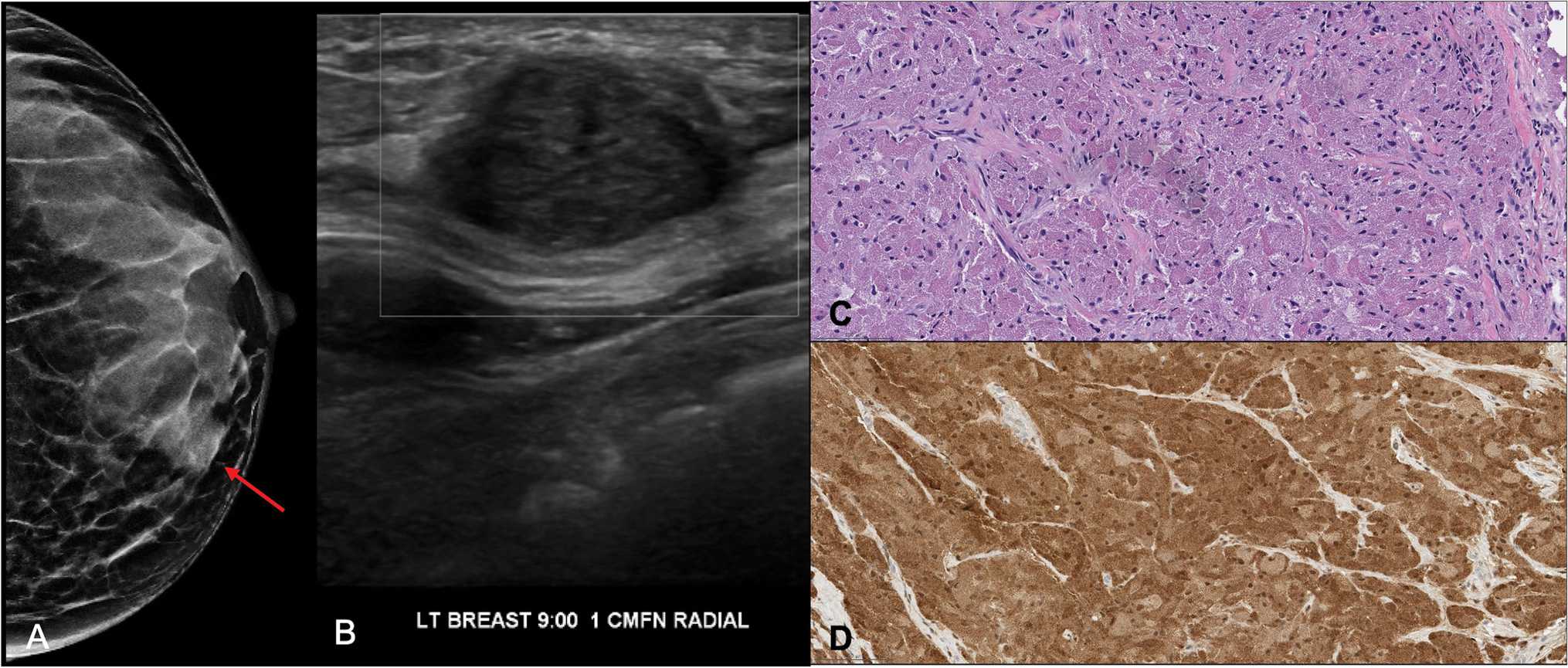
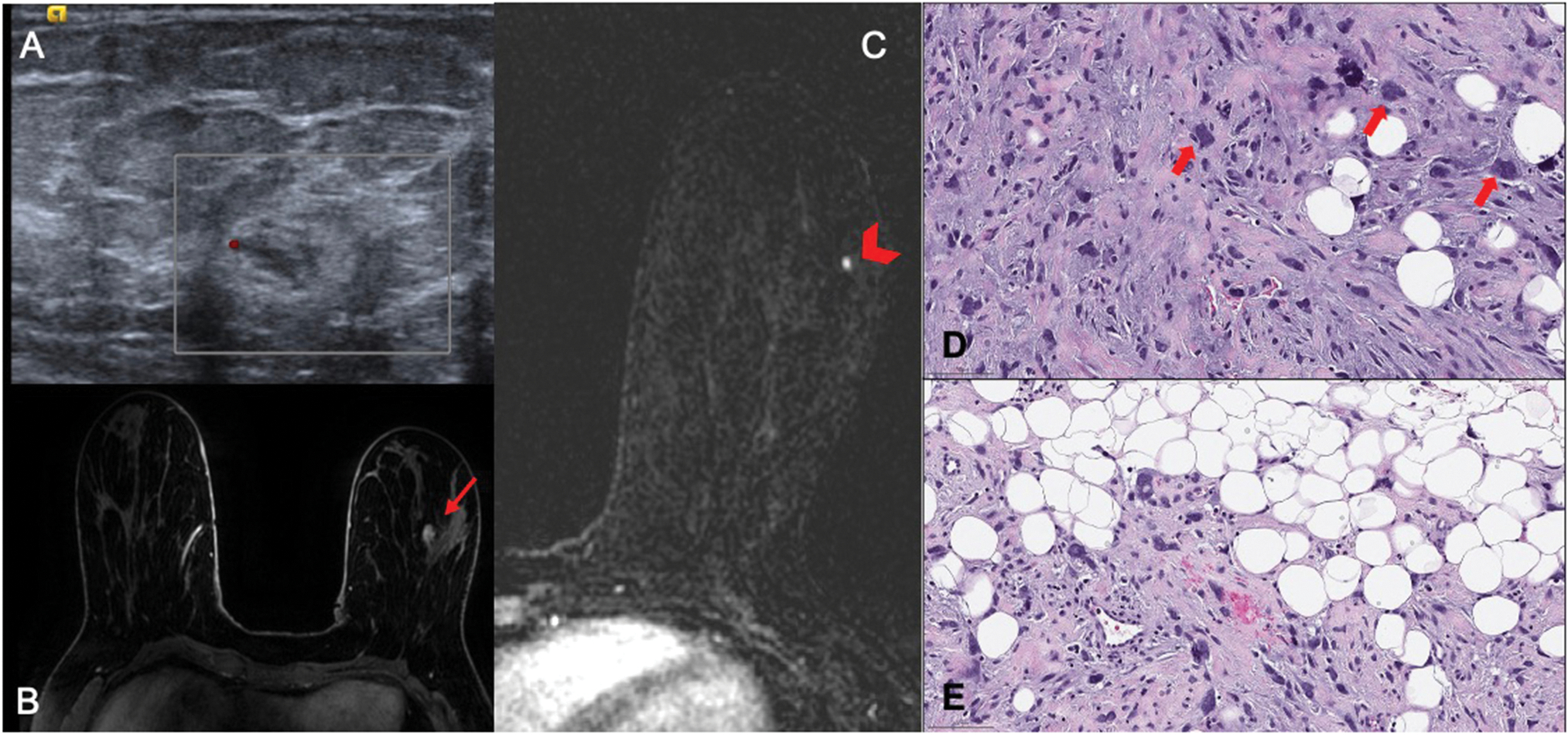
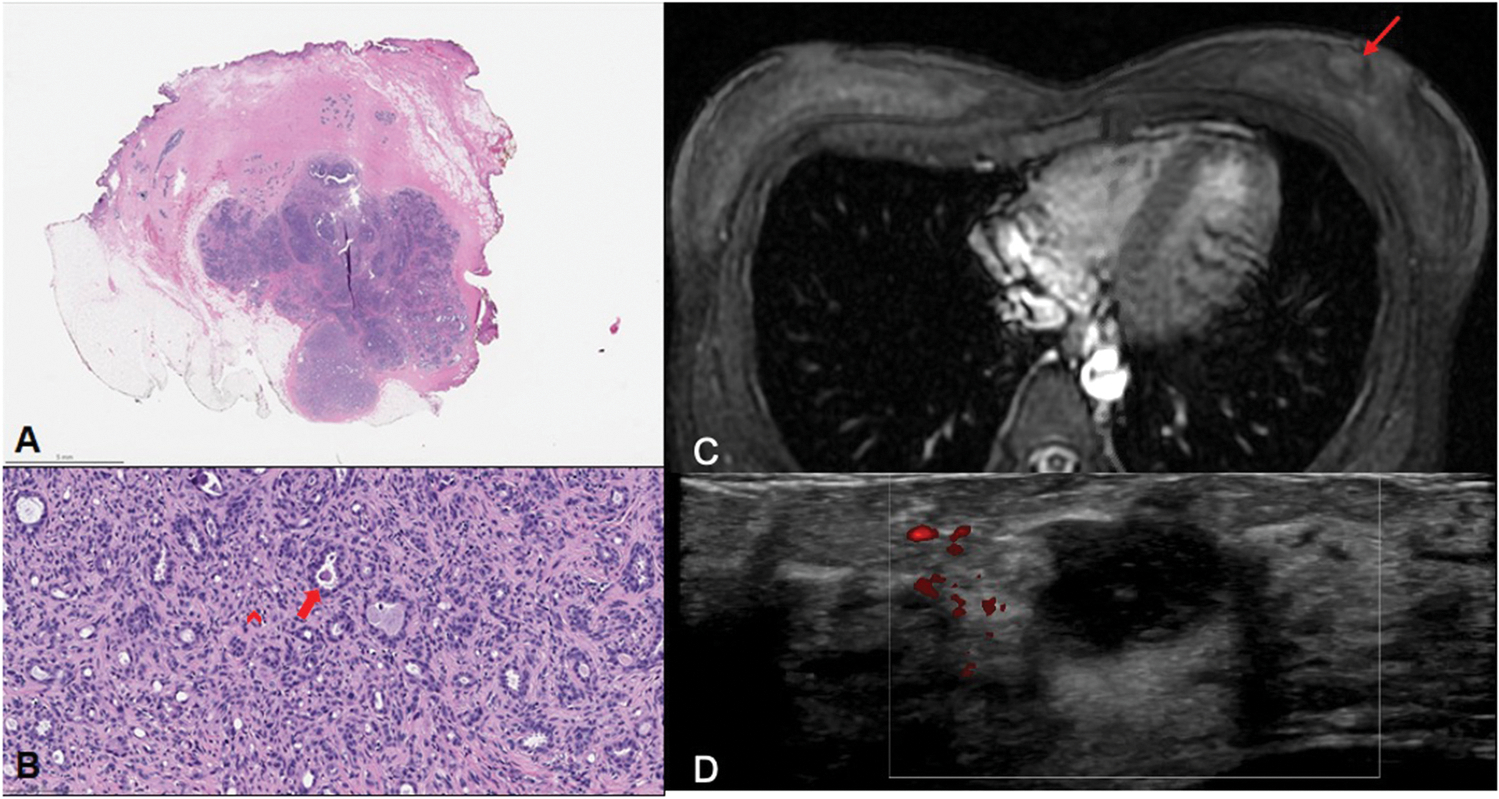
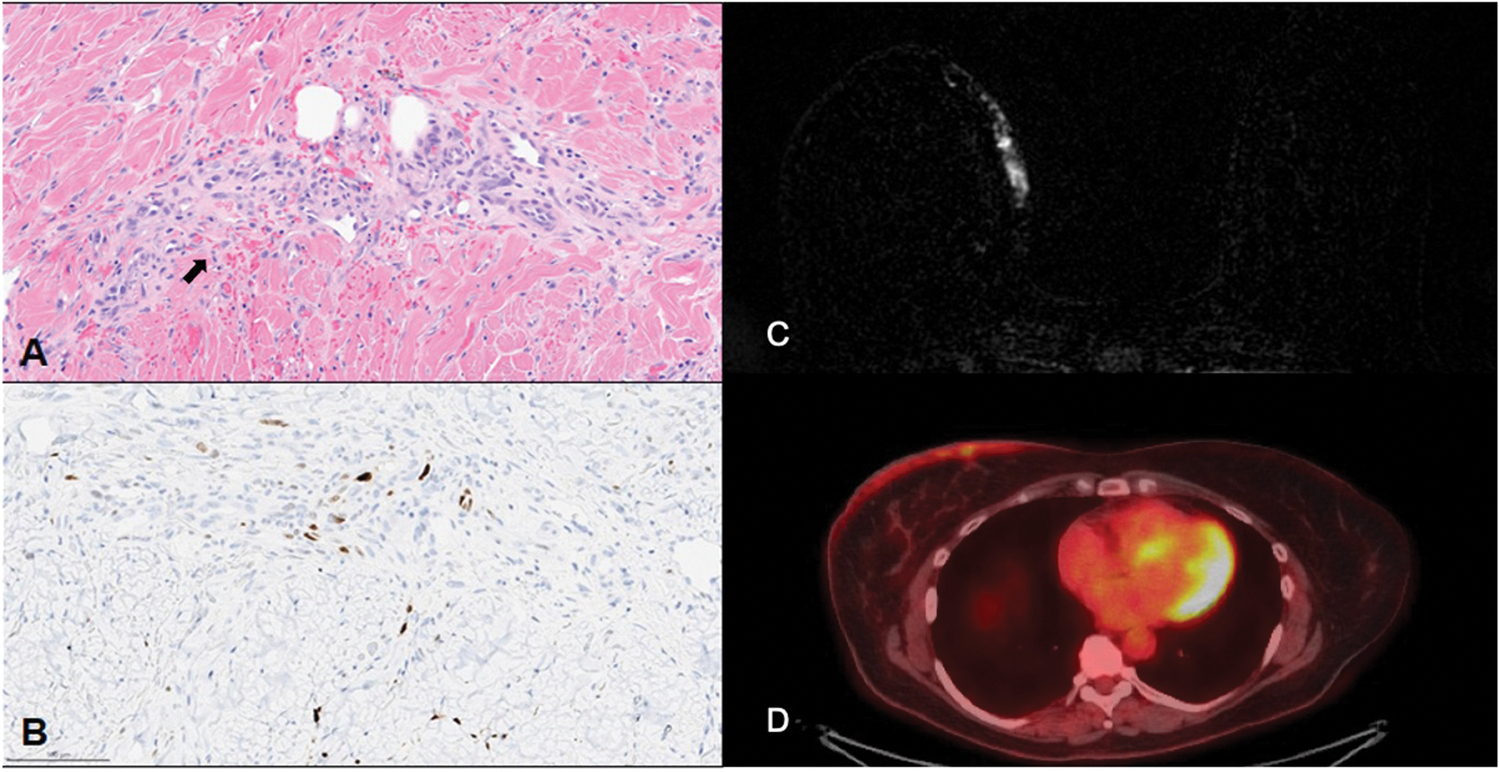
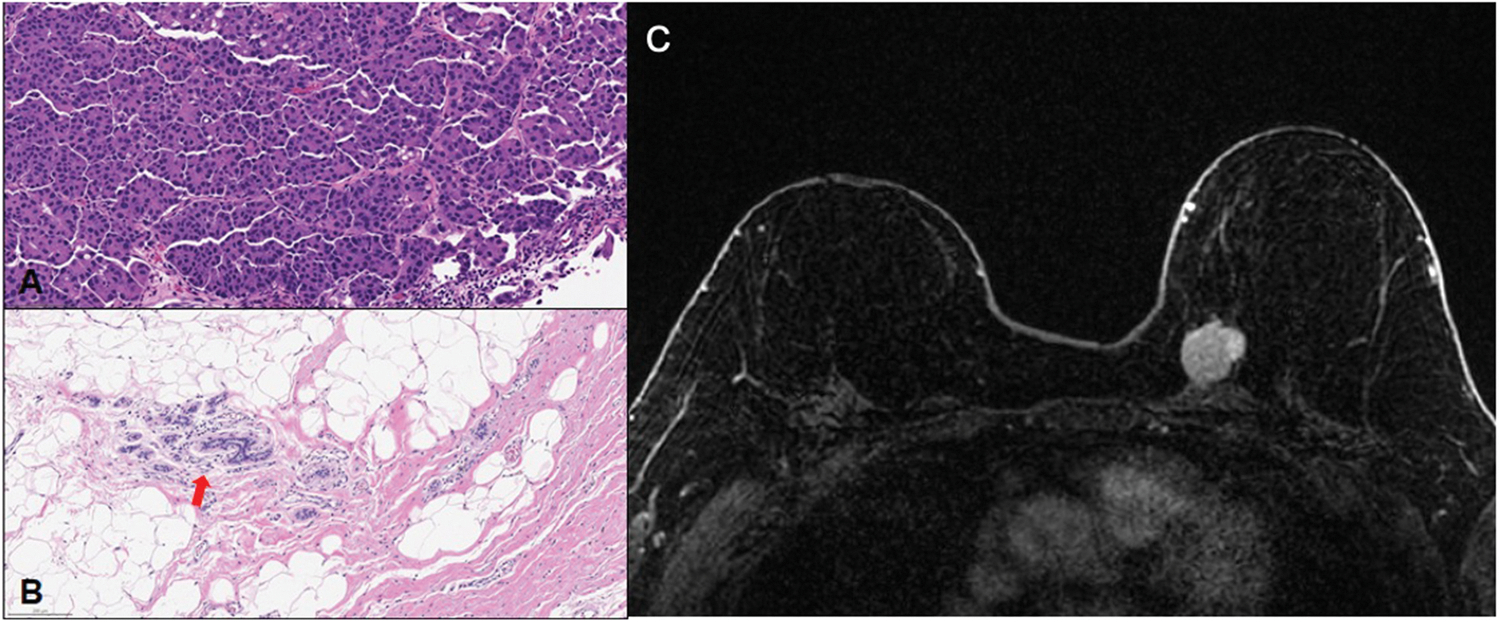
Purpose of review: The purpose is to present a case series of rare diagnoses and unusual presentations of breast lesions with radiologic-pathologic correlation from a major cancer center, and to review the recent literature on each entity with a focus on radiology-pathology concordance. We present our findings and experience from cases of metastatic small cell lung carcinoma to the breast, IgG-4 related breast disease, breast implant associated anaplastic large cell lymphoma, granular cell tumor, pleomorphic sarcoma, adenomyoepithelioma, post-radiation angiosarcoma, and breast carcinoma after risk-reducing total mastectomy.
Recent findings: It is essential for physicians to have knowledge of rare breast diagnoses and unusual breast disease presentations to formulate a complete differential diagnosis, recognize radiological-pathological concordance of these entities and provide appropriate patient care.
Summary: Current literature on these rare described entities exists mainly as case reports, case series and small-scale studies. By sharing our findings, we hope to educate trainees in radiology, pathology and other fields across the continuum of care in radiologic-pathologic correlation, while also augmenting the existing literature on these rare entities.
Keywords: Extramammary metastasis to breast; IgG4 related disease; adenomyoepithelioma; breast implant associated anaplastic large cell lymphoma; granular cell tumor; risk-reducing total mastectomy; sarcoma.
Conflict of interest statement
Conflict of Interest Marina Corines, Melissa Krystel-Whittemore, and Melissa Murray declare that they have no conflict of interest. Victoria Mango reports personal fees from Bayer Healthcare, personal fees from Koios Medical, outside the submitted work.
Figures
Similar articles
-
Breast adenomyoepithelioma and adenomyoepithelioma with carcinoma (malignant adenomyoepithelioma) with associated breast malignancies: A case series emphasizing histologic, radiologic, and clinical correlation.Breast. 2016 Oct;29:132-9. doi: 10.1016/j.breast.2016.07.018. Epub 2016 Aug 3. Breast. 2016. PMID: 27494340
-
Breast Implant-Associated Anaplastic Large Cell Lymphoma: A Case Report and Literature Review.Cureus. 2016 Mar 26;8(3):e546. doi: 10.7759/cureus.546. Cureus. 2016. PMID: 27158575 Free PMC article.
-
Combination of Adenomyoepithelioma and Adenoid Cystic Carcinoma of the Breast: A Case Report of an Uncommon Histopathological Entity.Am J Case Rep. 2022 Jan 22;23:e934391. doi: 10.12659/AJCR.934391. Am J Case Rep. 2022. PMID: 35064096 Free PMC article.
-
Spectrum of Extramammary Malignant Neoplasms in the Breast With Radiologic-Pathologic Correlation.Curr Probl Diagn Radiol. 2016 Nov-Dec;45(6):392-401. doi: 10.1067/j.cpradiol.2015.07.012. Epub 2015 Jul 30. Curr Probl Diagn Radiol. 2016. PMID: 26416136 Review.
-
Anaplastic large cell lymphoma occurring in association with breast implants: review of pathologic and immunohistochemical features in 103 cases.Appl Immunohistochem Mol Morphol. 2013 Jan;21(1):13-20. doi: 10.1097/PAI.0b013e318266476c. Appl Immunohistochem Mol Morphol. 2013. PMID: 23235342 Review.
Cited by
-
IgG4-related Breast Disease: Review of the Literature.Rambam Maimonides Med J. 2024 Oct 28;15(4):e0018. doi: 10.5041/RMMJ.10532. Rambam Maimonides Med J. 2024. PMID: 39503548 Free PMC article. Review.
-
Detection of benign granular cell tumor of the breast via 18F-PSMA-PET/CT in a patient with very high-risk prostate cancer: A case report.SAGE Open Med Case Rep. 2024 Aug 31;12:2050313X241275826. doi: 10.1177/2050313X241275826. eCollection 2024. SAGE Open Med Case Rep. 2024. PMID: 39224763 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials