

Leadless biventricular left bundle and endocardial lateral wall pacing versus left bundle only pacing in left bundle branch block patients
- PMID: 36589454
- PMCID: PMC9794756
- DOI: 10.3389/fphys.2022.1049214
Leadless biventricular left bundle and endocardial lateral wall pacing versus left bundle only pacing in left bundle branch block patients
Abstract
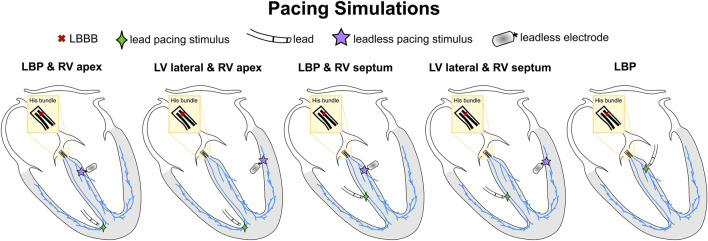
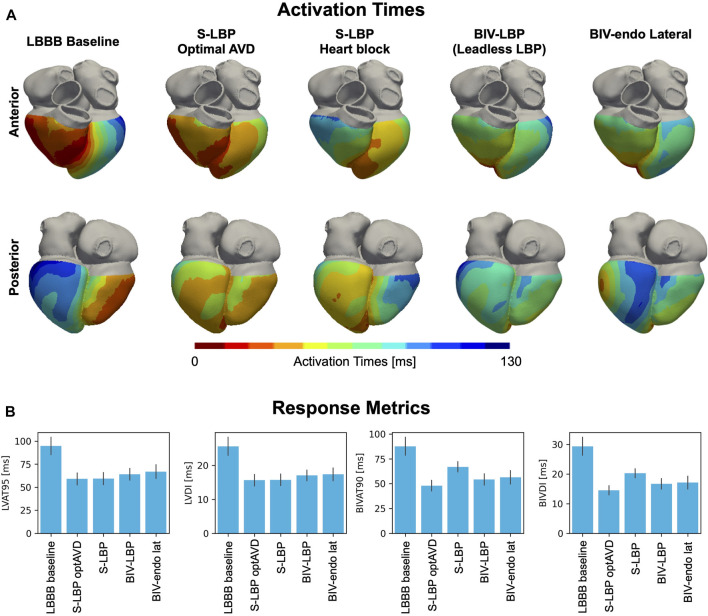
Biventricular endocardial (BIV-endo) pacing and left bundle pacing (LBP) are novel delivery methods for cardiac resynchronization therapy (CRT). Both pacing methods can be delivered through leadless pacing, to avoid risks associated with endocardial or transvenous leads. We used computational modelling to quantify synchrony induced by BIV-endo pacing and LBP through a leadless pacing system, and to investigate how the right-left ventricle (RV-LV) delay, RV lead location and type of left bundle capture affect response. We simulated ventricular activation on twenty-four four-chamber heart meshes inclusive of His-Purkinje networks with left bundle branch block (LBBB). Leadless biventricular (BIV) pacing was simulated by adding an RV apical stimulus and an LV lateral wall stimulus (BIV-endo lateral) or targeting the left bundle (BIV-LBP), with an RV-LV delay set to 5 ms. To test effect of prolonged RV-LV delays and RV pacing location, the RV-LV delay was increased to 35 ms and/or the RV stimulus was moved to the RV septum. BIV-endo lateral pacing was less sensitive to increased RV-LV delays, while RV septal pacing worsened response compared to RV apical pacing, especially for long RV-LV delays. To investigate how left bundle capture affects response, we computed 90% BIV activation times (BIVAT-90) during BIV-LBP with selective and non-selective capture, and left bundle branch area pacing (LBBAP), simulated by pacing 1 cm below the left bundle. Non-selective LBP was comparable to selective LBP. LBBAP was worse than selective LBP (BIVAT-90: 54.2 ± 5.7 ms vs. 62.7 ± 6.5, p < 0.01), but it still significantly reduced activation times from baseline. Finally, we compared leadless LBP with RV pacing against optimal LBP delivery through a standard lead system by simulating BIV-LBP and selective LBP alone with and without optimized atrioventricular delay (AVD). Although LBP alone with optimized AVD was better than BIV-LBP, when AVD optimization was not possible BIV-LBP outperformed LBP alone, because the RV pacing stimulus shortened RV activation (BIVAT-90: 54.2 ± 5.7 ms vs. 66.9 ± 5.1 ms, p < 0.01). BIV-endo lateral pacing or LBP delivered through a leadless system could potentially become an alternative to standard CRT. RV-LV delay, RV lead location and type of left bundle capture affect leadless pacing efficacy and should be considered in future trial designs.
Keywords: cardiac resynchronization therapy; conduction system pacing; dyssynchrony; endocardial pacing; leadless pacing; left bundle branch block; left bundle pacing.
Copyright © 2022 Strocchi, Wijesuriya, Elliott, Gillette, Neic, Mehta, Vigmond, Plank, Rinaldi and Niederer.
Conflict of interest statement
AN is employed by NumeriCor GmbH, Graz, Austria. The remaining authors declare that the research was conducted in the absence of any commercial of financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Arnold A. D., Shun-Shin M. J., Keene D., Howard J. P., Afzal Sohaib S. M., Wright I. J., et al. (2018). His resynchronization therapy vs. biventricular pacing for heart failure with LBBB: A within-patient comparison of effects on acute haemodynamic function and ventricular activation. Europace 20 (Suppl. 4), iv25. 10.1093/europace/euy201.001 - DOI
-
- Auricchio A., Delnoy P. P., Butter C., Brachmann J., van Erven L., Spitzer S., et al. (2014). Feasibility, safety, and short-term outcome of leadless ultrasound-based endocardial left ventricular resynchronization in heart failure patients: Results of the Wireless Stimulation Endocardially for CRT (WiSE-CRT) study. Europace 16, 681–688. 10.1093/europace/eut435 - DOI - PubMed
-
- Bazoukis G., Naka K. K., Alsheikh-Ali A., Tse G., Letsas K. P., Korantzopoulos P., et al. (2020). Association of QRS narrowing with response to cardiac resynchronization therapy—A systematic review and meta-analysis of observational studies. Heart fail. Rev. 25, 745–756. 10.1007/s10741-019-09839-5 - DOI - PubMed
-
- Behar J. M., Jackson T., Hyde E., Claridge S., Gill J., Bostock J., et al. (2016). Optimized left ventricular endocardial stimulation is superior to optimized epicardial stimulation in ischemic patients with poor response to cardiac resynchronization therapy: A combined magnetic resonance imaging, electroanatomic contact mapping, and hemodynamic study to target endocardial lead placement. JACC. Clin. Electrophysiol. 2, 799–809. 10.1016/j.jacep.2016.04.006 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous