

Multimodal imaging approach in hyponatremic hypertensive syndrome. A rare case of pediatric unilateral hypoplasia of the main renal artery combined itself with stenosis and review of literature
- PMID: 36589503
- PMCID: PMC9798128
- DOI: 10.1016/j.radcr.2022.10.034
Multimodal imaging approach in hyponatremic hypertensive syndrome. A rare case of pediatric unilateral hypoplasia of the main renal artery combined itself with stenosis and review of literature
Abstract
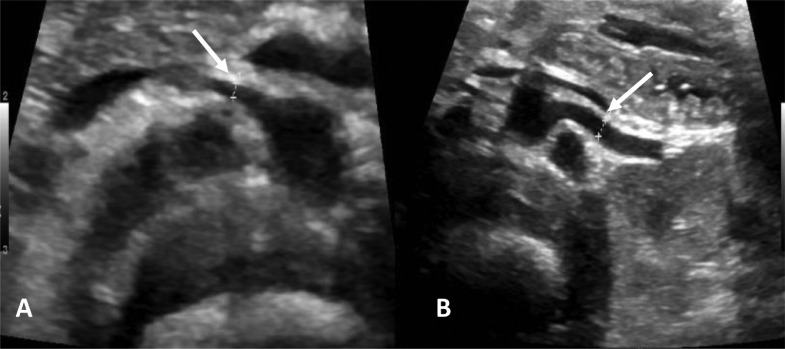
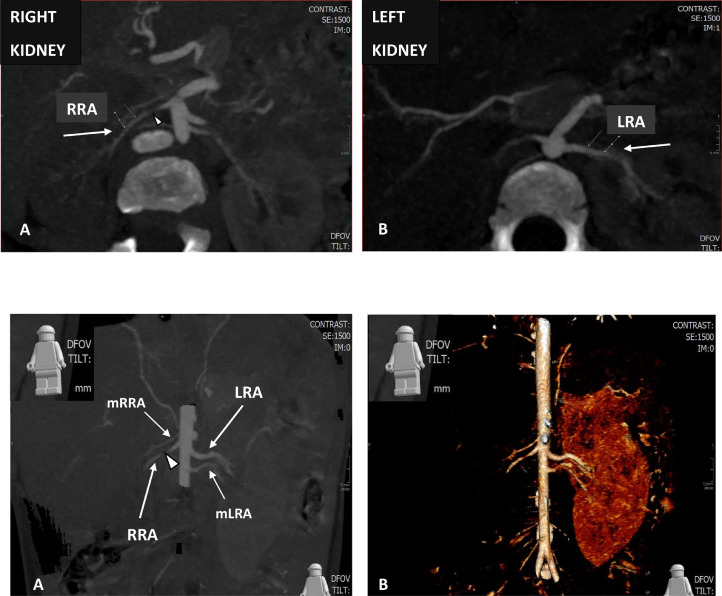
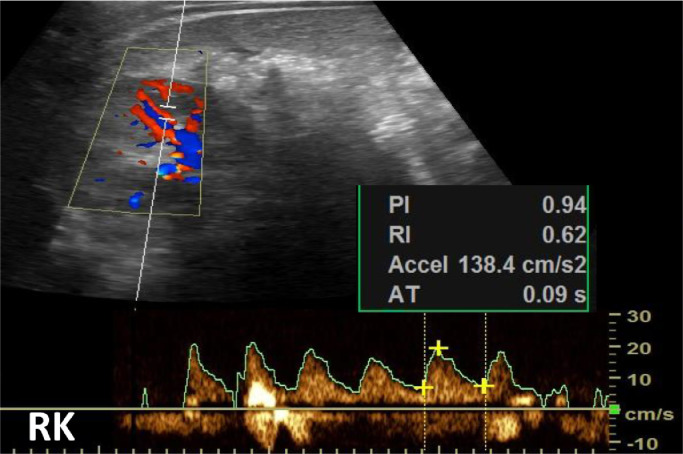
Renal artery stenosis (RAS) accounts for approximately 5%-10% of secondary renovascular hypertension in the pediatric population. It can occur as an isolated entity, or as a hypoplasia combined itself with stenosis. Hypoplasia, or long-segment developmental narrowing, is a rare cause of renovascular hypertension. Hyponatremic hypertensive syndrome (HHS) is a malignant complication of unilateral RAS and/or renal artery hypoplasia. Hyponatremia, hypokalemic hypochloremic metabolic alkalosis, nephrotic range proteinuria, polyuria, polydipsia, and weight loss are the most common findings. In particular, hypertension remains refractory despite aggressive antihypertensive therapy. Laboratory findings of elevated plasma levels of renin in most case suggest that the stimulation of renin release from the ischemic kidney plays an important pathophysiologic role. HHS is a diagnostic and therapeutic challenge in children. We report a case of a unilateral right renal artery hypoplasia, complicated by a segmental narrowing, in a 17-month-old male, clinically symptomatic for hypertension. We emphasize the role of ultrasound, computed tomography, and digital subtraction angiography that should be planned as reliable and non-invasive multimodal imaging approach.
Keywords: Angioplasty; Computed tomography angiography; Hyponatremic hypertensive syndrome; Hypoplasia; Renovascular hypertension; Ultrasound.
© 2022 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures





References
-
- Vo NJ, Hammelman BD, Racadio JM, Strife CF, Johnson ND, Racadio JM, et al. Anatomic distribution of renal artery stenosis in children: implications for imaging. Pediatr Radiol. 2006;36:1032–1036. - PubMed
-
- Slovut DP, Olin JW. Fibromuscular dysplasia. N Eng J Med. 2004;350:1862–1871. - PubMed
-
- Lin YL, Hwang B, Lee PC, Yang Ling-Yu, Laura Meng CC, et al. Mid-aortic syndrome: a case report and review of the literature. Int J Cardiol. 2008;123(3):348–352. - PubMed
-
- Sahoo B, Patnaik S. Ask-Upmark kidney: renovascular hypertension in a child. A case report. J Med Res. 2015;1(3):81–82.
-
- Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001;344(6):431–442. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
