

A Multisite Assessment of Inpatient Safety Event Rates During the Coronavirus Disease 2019 Pandemic
- PMID: 36590139
- PMCID: PMC9790867
- DOI: 10.1016/j.mayocpiqo.2022.12.004
A Multisite Assessment of Inpatient Safety Event Rates During the Coronavirus Disease 2019 Pandemic
Abstract
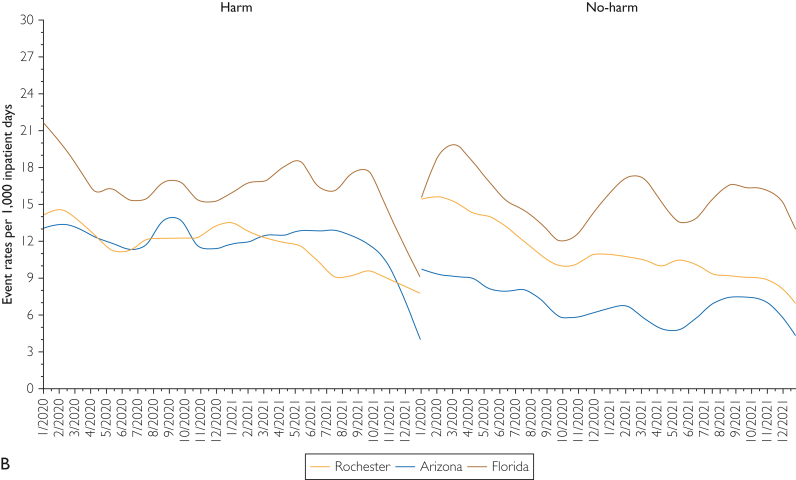
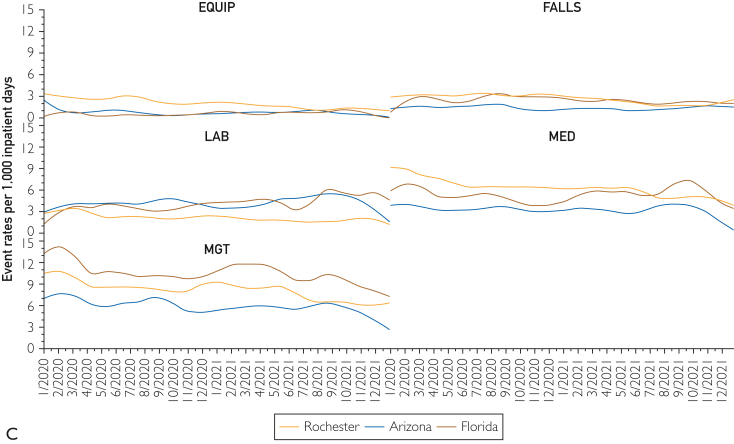
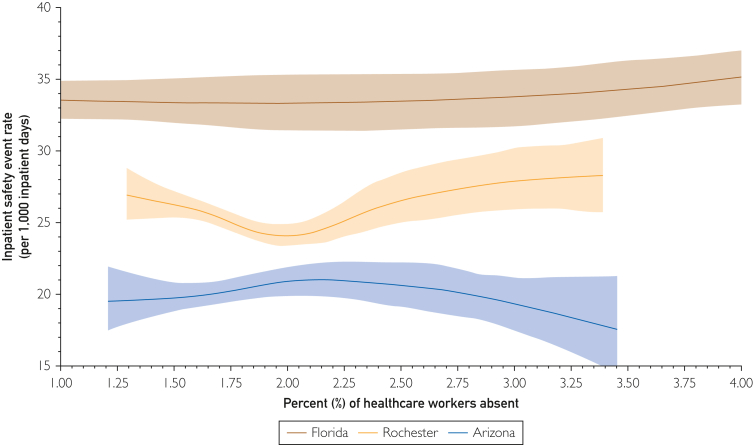
To date, there has been a notable lack of peer-reviewed or publicly available data documenting rates of hospital quality outcomes and patient safety events during the coronavirus disease 2019 pandemic era. The dearth of evidence is perhaps related to the US health care system triaging resources toward patient care and away from reporting and research and also reflects that data used in publicly reported hospital quality rankings and ratings typically lag 2-5 years. At our institution, a learning health system assessment is underway to evaluate how patient safety was affected by the pandemic. Here we share and discuss early findings, noting the limitations of self-reported safety event reporting, and suggest the need for further widespread investigations at other US hospitals. During the 2-year study period from January 1, 2020, through December 31, 2021 across 3 large US academic medical centers at our institution, we documented an overall rate of 25.8 safety events per 1000 inpatient days. The rate of events meeting "harm" criteria was 12.4 per 1000 inpatient days, the rate of nonharm events was 11.1 per 1000 inpatient days, and the fall rate was 2.3 per 1000 inpatient days. This descriptive exploratory analysis suggests that patient safety event rates at our institution did not increase over the course of the pandemic. However, increasing health care worker absences were nonlinearly and strongly associated with patient safety event rates, which raises questions regarding the mechanisms by which patient safety event rates may be affected by staff absences during pandemic peaks.
Keywords: AHRQ, Agency for Healthcare Research and Quality; COVID-19, coronavirus disease 2019; PSI, Patient Safety Indicator.
© 2022 The Authors.
Figures

References
-
- AHRQ national scorecard on hospital-acquired conditions updated baseline rates and preliminary results 2014–2017 Agency for Healthcare Research and Quality. https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-p... Published January 2019.
-
- Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the long-term care hospital prospective payment system and policy changes and fiscal year 2022 rates; quality programs and Medicare promoting interoperability program requirements for eligible hospitals and critical access hospitals; changes to Medicaid provider enrollment; and changes to the Medicare shared savings program. 86 FR 44774. Centers for Medicare and Medicaid Services. Published August 13, 2021. Accessed June 14 2022. https://www.federalregister.gov/documents/2021/08/13/2021-16519/medicare...
-
- Weiner-Lastinger L.M., Pattabiraman V., Konnor R.Y., et al. The impact of coronavirus disease 2019 (COVID-19) on healthcare-associated infections in 2020: a summary of data reported to the National Healthcare Safety Network. Infect Control Hosp Epidemiol. 2022;43(1):12–25. - PubMed
LinkOut - more resources
Full Text Sources
