

Comparison of outcomes of retrograde intramedullary nailing versus locking plate fixation in distal femur fractures: A Systematic Review and Meta-analysis of 936 patients in 16 studies
- PMID: 36591439
- PMCID: PMC9800249
- DOI: 10.1016/j.jor.2022.12.007
Comparison of outcomes of retrograde intramedullary nailing versus locking plate fixation in distal femur fractures: A Systematic Review and Meta-analysis of 936 patients in 16 studies
Abstract
Background: The surgical treatment for distal femur fractures has evolved over time, and it depends upon certain factors; open or closed fracture type, the pattern of fracture, presence of metaphyseal comminution, intra-articular extension, and the bone quality are some of the crucial ones. Both retrograde intramedullary nails (RIMN) and locking plates (LP) can be used for the fixation of these fractures. However, the optimal method among the two devices is still a topic of debate, the superiority of one over the other being unclear. Hence, this systematic review and meta-analysis was conceptualized to compare the outcomes of RIMN with distal femur LP.
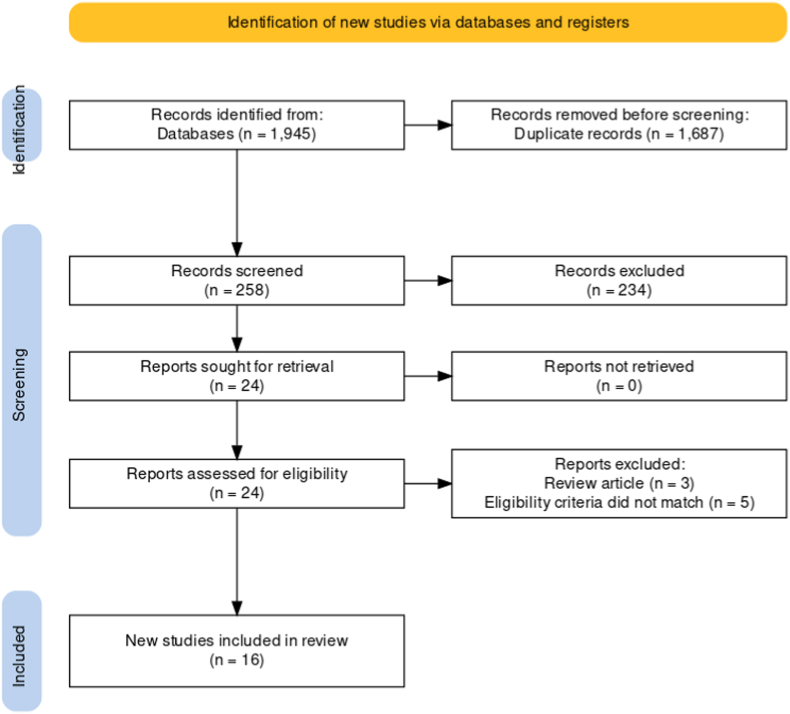
Methods: The primary electronic search was conducted on Medline (PubMed), Scopus, Embase, Cinahl, and Cochrane Library databases for the published literature from the inception to 25th February 2022. The studies compared outcomes of RIMN versus LP fixation of the acute supracondylar or distal femur fracture (AO/OTA type-33A, B, and C) and reported at least one primary (mean fracture union time, complications, implant-related complications, and re-operation rate) or secondary outcome (duration of surgery, intra-operative blood loss, and knee range of motion), were included.
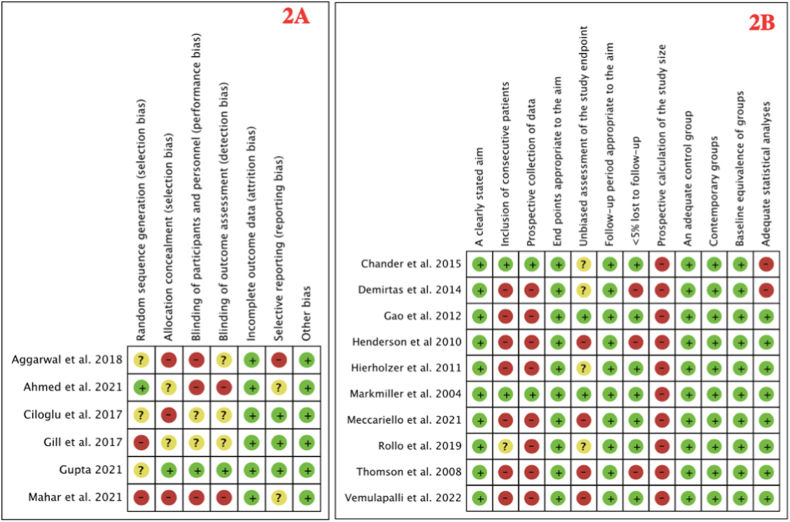
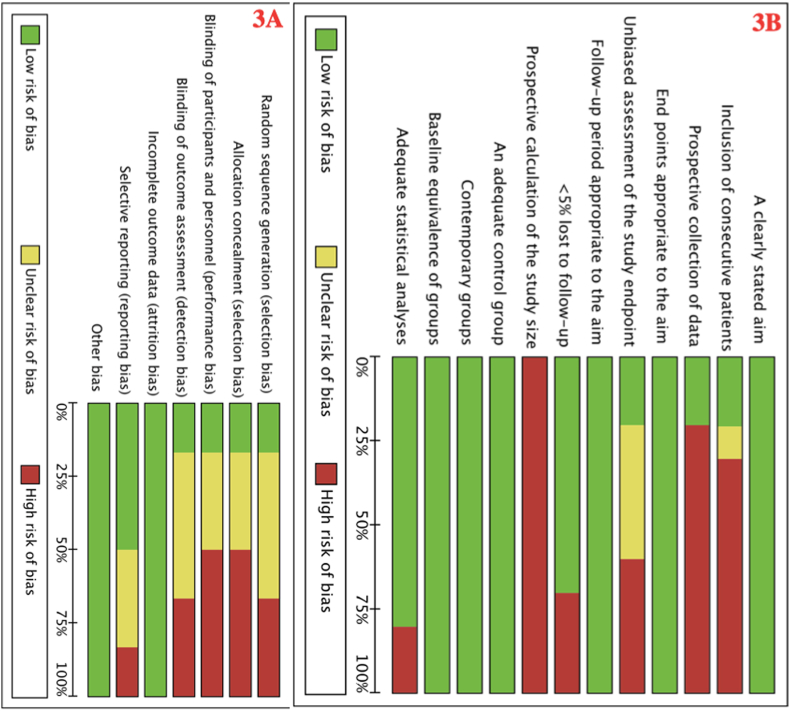
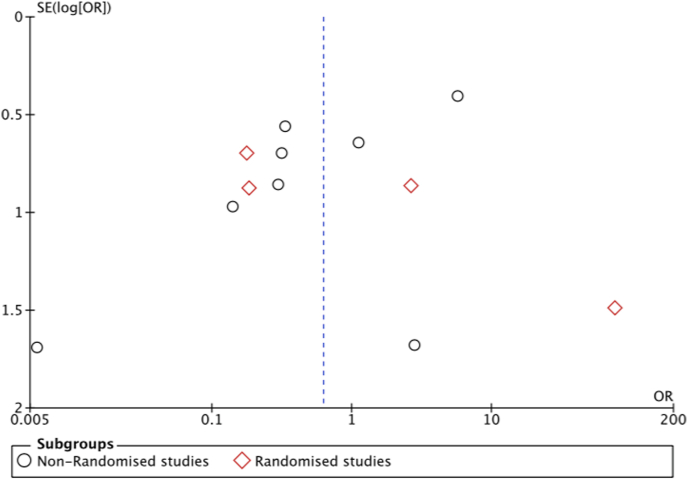
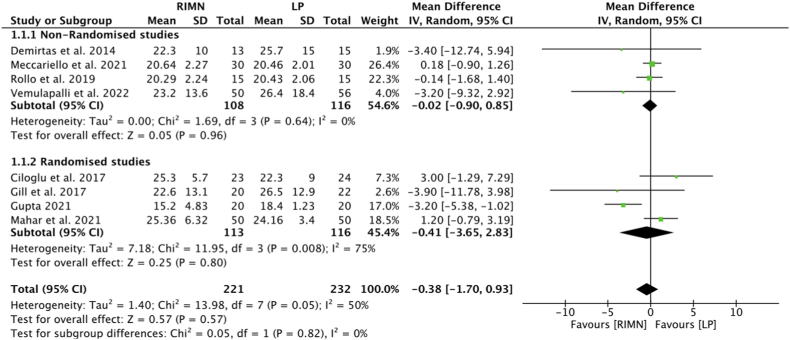
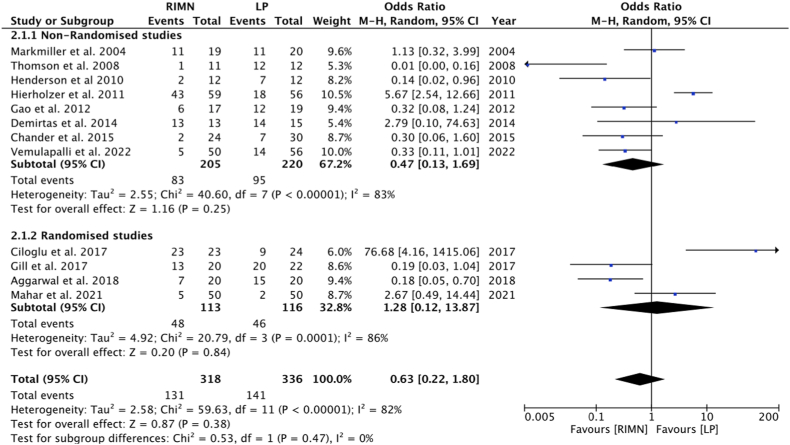
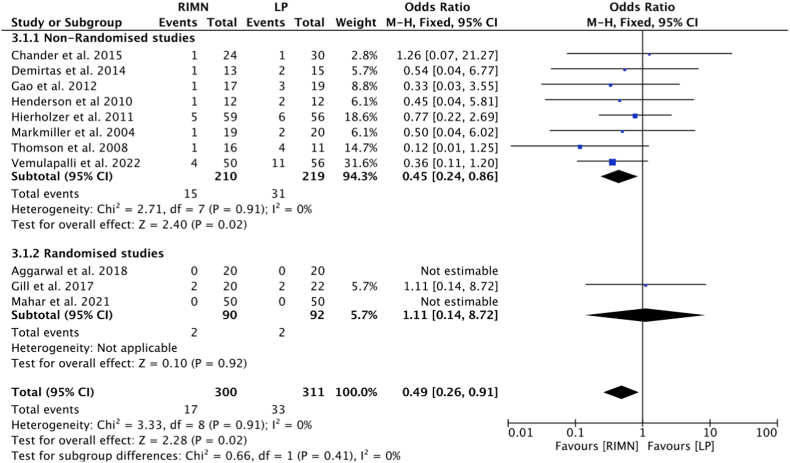
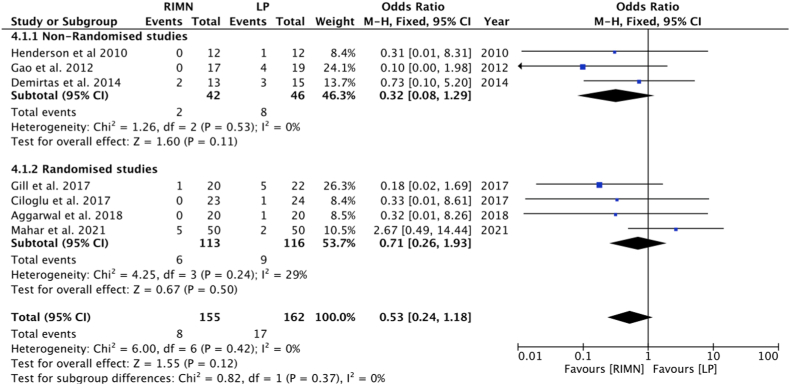
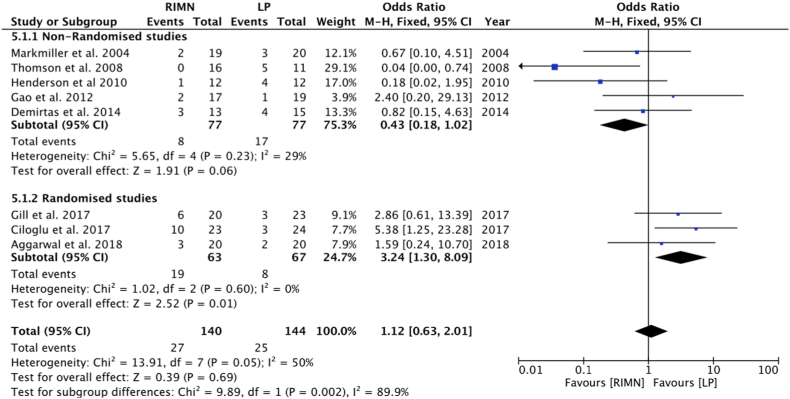
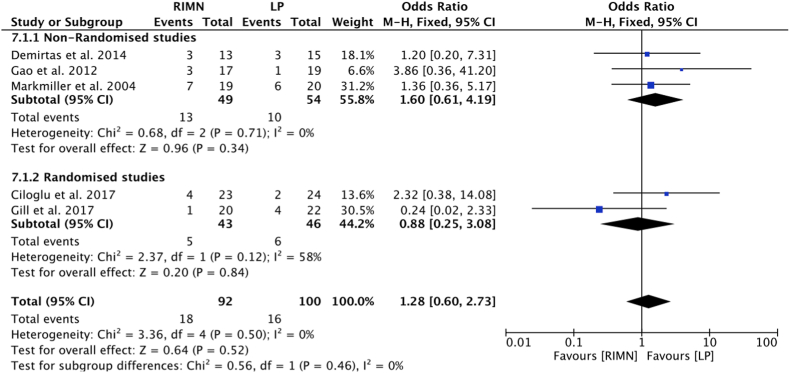
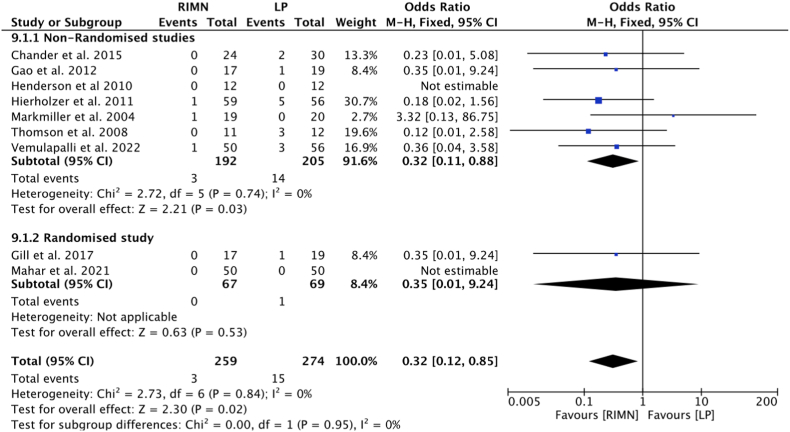
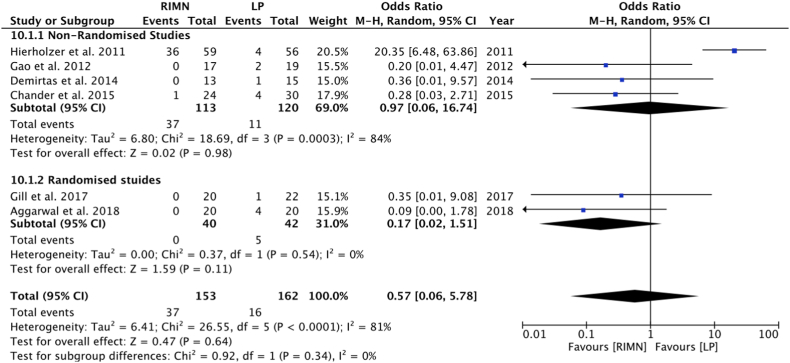
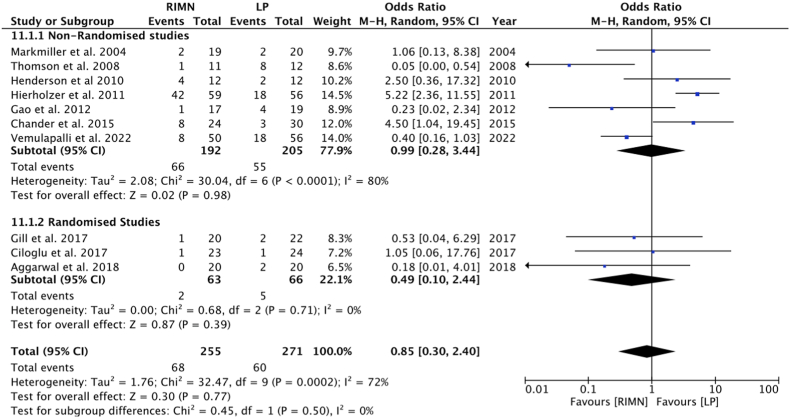
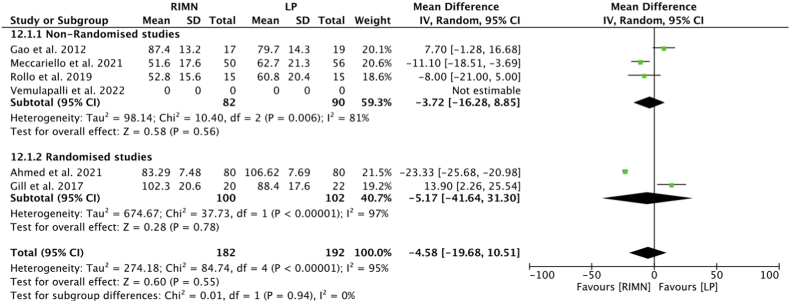
Results: Six randomized control trials, 2 prospective and 8 retrospective studies with 936 patients with 8 bilateral cases (467: RIMN; 477: LP) were included. Our analysis demonstrated no statistically significant difference in terms of mean fracture union time, overall complications, implant-related complications, re-operation rates, and duration of surgeries. Although a better knee range of motion was seen in the LP group, however, it also showed more nonunion and infection than the RIMN group.
Conclusion: The present review shows that there are significantly lesser nonunions and infections, in the RIMN group as compared to LP for distal femur fractures, although a better postoperative knee range of motion was seen in the latter. However, in terms of fracture union time, the overall rate of complications, re-operation rates, and duration of surgeries, there is no difference between the two surgical options.
Keywords: Distal femoral locking plate; Distal femoral nail; Distal femur fracture; Locking plate; Retrograde femoral nail; Supracondylar femur fracture.
© 2022 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Court-Brown C.M., Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37(8):691–697. - PubMed
-
- Gwathmey F.W., Jr., Jones-Quaidoo S.M., Kahler D., Hurwitz S., Cui Q. Distal femoral fractures: current concepts. J Am Acad Orthop Surg. 2010;18(10):597–607. - PubMed
-
- Zlowodzki M., Bhandari M., Marek D.J., Cole P.A., Kregor P.J. Operative treatment of acute distal femur fractures: systematic review of two comparative studies and 45 case series (1989-2005) J Orthop Trauma. 2006;20:366–371. - PubMed
-
- Walcher F., Frank J., Marzi I. Retrogradenailing of distal femoral fracture–clear andpotential indications. Eur J Trauma. 2000;26(4):155–168.
-
- Wenger D., Andersson S. Low risk of nonunion with lateral locked plating of distal femoral fractures-A retrospective study of 191 consecutive patients. Injury. 2019;50(2):448–452. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
