

Multisite ALLFTD study modeling progressive empathy loss from the earliest stages of behavioral variant frontotemporal dementia
- PMID: 36591730
- PMCID: PMC10314956
- DOI: 10.1002/alz.12898
Multisite ALLFTD study modeling progressive empathy loss from the earliest stages of behavioral variant frontotemporal dementia
Abstract
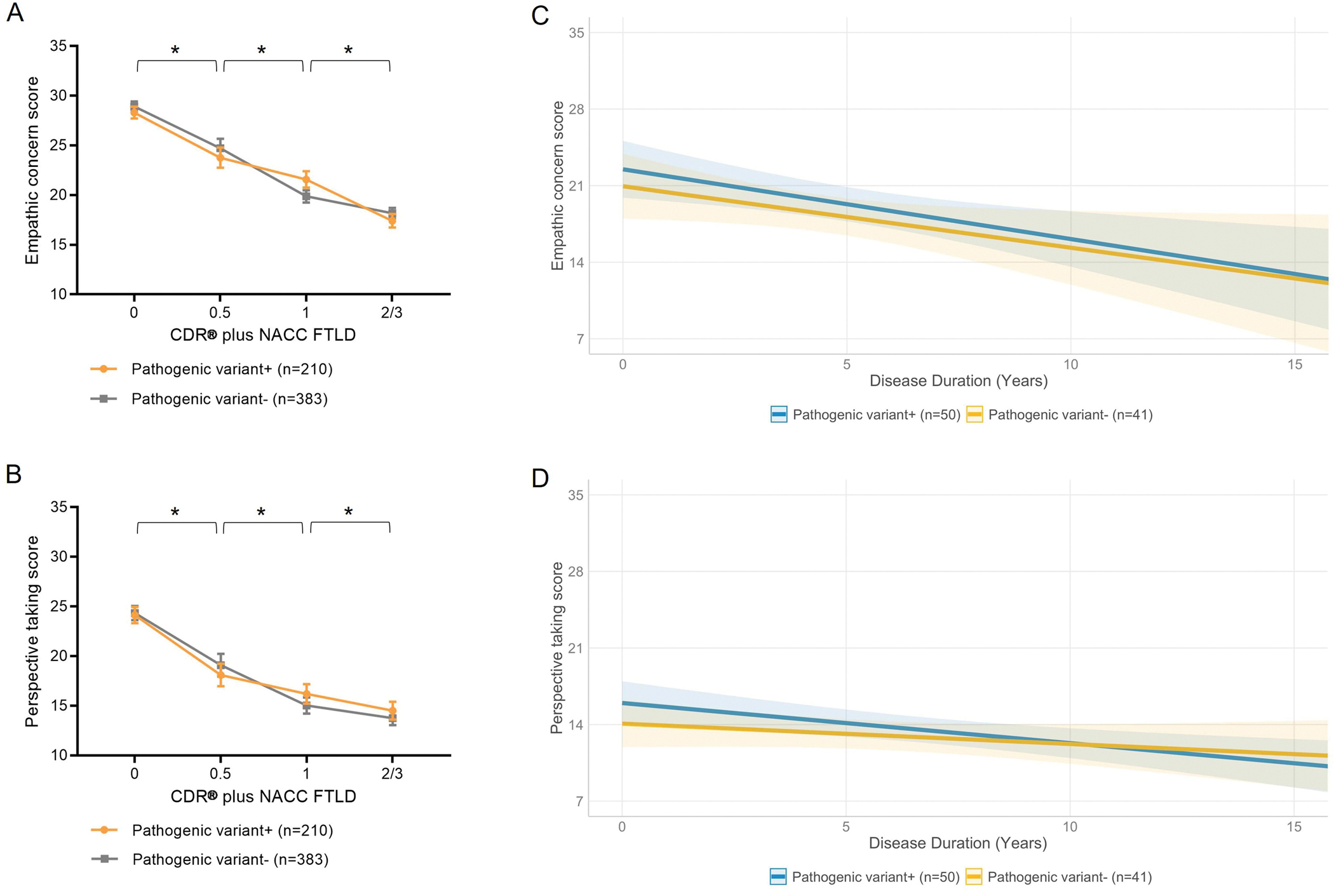
Introduction: Empathy relies on fronto-cingular and temporal networks that are selectively vulnerable in behavioral variant frontotemporal dementia (bvFTD). This study modeled when in the disease process empathy changes begin, and how they progress.
Methods: Four hundred thirty-one individuals with asymptomatic genetic FTD (n = 114), genetic and sporadic bvFTD (n = 317), and 163 asymptomatic non-carrier controls were enrolled. In sub-samples, we investigated empathy measured by the informant-based Interpersonal Reactivity Index (IRI) at each disease stage and over time (n = 91), and its correspondence to underlying atrophy (n = 51).
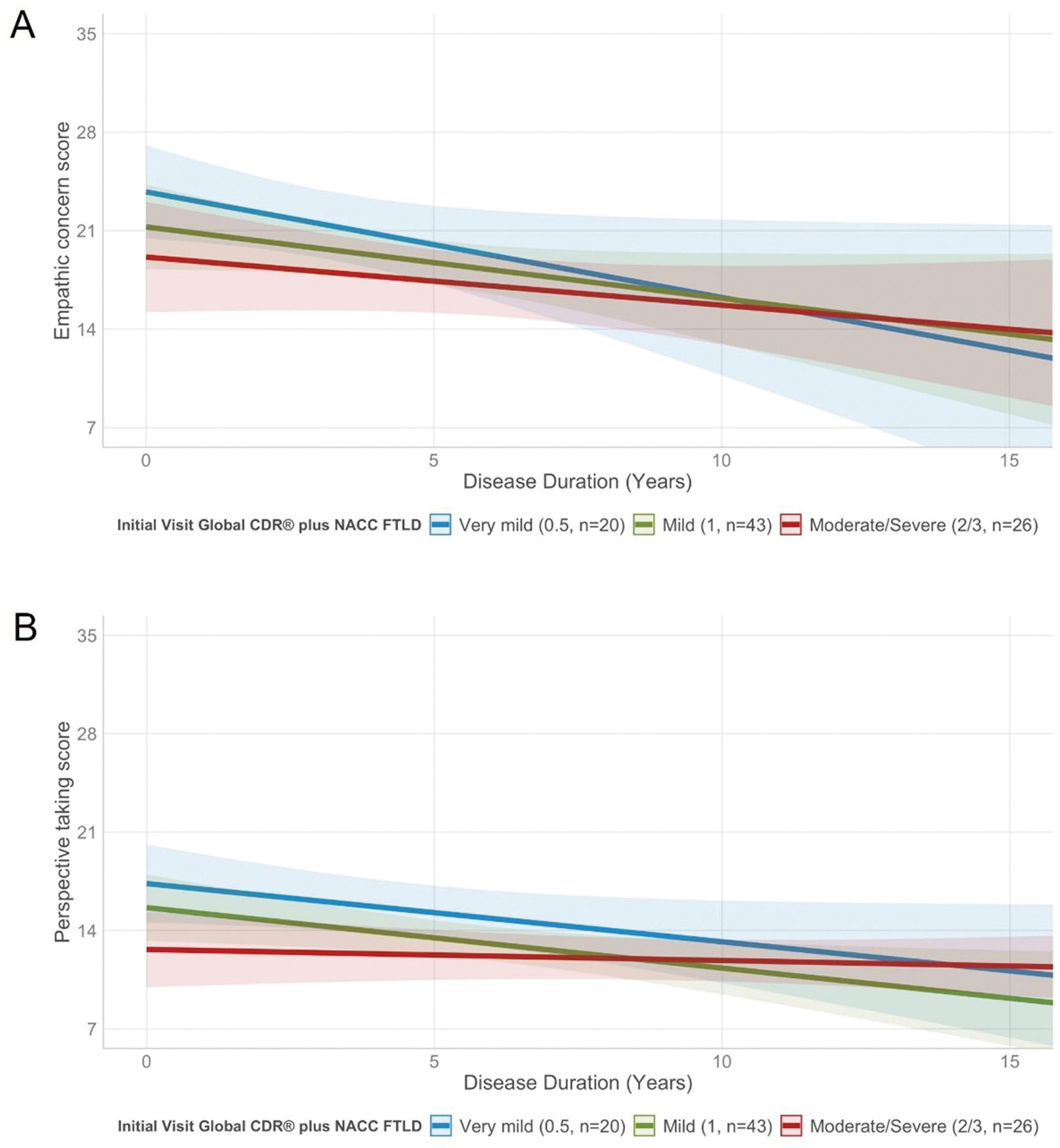
Results: Empathic concern (estimate = 4.38, 95% confidence interval [CI] = 2.79, 5.97; p < 0.001) and perspective taking (estimate = 5.64, 95% CI = 3.81, 7.48; p < 0.001) scores declined between the asymptomatic and very mild symptomatic stages regardless of pathogenic variant status. More rapid loss of empathy corresponded with subcortical atrophy.
Discussion: Loss of empathy is an early and progressive symptom of bvFTD that is measurable by IRI informant ratings and can be used to monitor behavior in neuropsychiatry practice and treatment trials.
Keywords: Interpersonal Reactivity Index; behavioral variant frontotemporal dementia; clinical trials; cognitive empathy; emotional empathy; volumetric MRI.
© 2022 the Alzheimer's Association.
Conflict of interest statement
POTENTIAL CONFLICTS OF INTEREST
GT: research support from the Swiss National Science Foundation.
YC: the author reports no disclosures relevant to this manuscript.
PC: the author reports no disclosures relevant to this manuscript.
BSA: research support from CDC, NIH, and Ionis.
DB: the author reports no disclosures relevant to this manuscript.
KDR: research support from NIH. She has served as an investigator for clinical trials sponsored by Avid Radiopharmaceuticals, Biogen, and Janssen Pharmaceuticals and has served as Advisory Board consultant for Biogen.
LKF: the author reports no disclosures relevant to this manuscript.
NG: research support from NIH, the Association for Frontotemporal Degeneration, Tau Consortium. She has participated in multicenter therapy studies by sponsored by Bristol Myers Squibb, Lilly, Janssen, Novartis, Pfizer, Wyeth.
JGR: receives funding from NIH and serves on editorial board for Neurology.
NRGR: receives royalties from UpToDate, has participated in multicenter therapy studies by sponsored by Biogen, TauRx, AbbVie, Novartis and Lilly. He receives research support from NIH.
MG: receives research support from NIH, Avid and Piramal. He participates in clinical trials sponsored by Biogen, TauRx, and Alector, serves as a consultant to Bracco and UCB, and serves on the Editorial Board of Neurology.
HWH: the author reports no disclosures relevant to this manuscript.
JK: the author reports no disclosures relevant to this manuscript.
WK: receives research funding from AstraZeneca, Biogen, Roche, DOD and NIH.
MIL: research support from NIH.
GL: the author reports no disclosures relevant to this manuscript.
IL: research is supported by the National Institutes of Health grants: 5P50AG005131-33, 2R01AG038791-06A, U01NS090259, U01NS100610, U01NS80818, R25NS098999, P20GM109025; U19 AG063911-1; Parkinson Study Group, Michael J Fox Foundation, Parkinson Foundation, Lewy Body Association, Roche, Abbvie, Biogen, EIP-Pharma and Biohaven Pharmaceuticals. IL was member of a Lundbeck Advisory Board and participated in a symposium organized by Sunovion. IL receives her salary from the University of California San Diego and as Chief Editor of Frontiers in Neurology.
IRM: has been a paid member of the Scientific Advisory Board for Prevail Therapeutics.
BP: the author reports no disclosures relevant to this manuscript.
EMR: the author reports no disclosures relevant to this manuscript.
KR: research support from NIH.
JCR: receives research support from NIH-NIA. He is a site PI for clinical trials sponsored by Eli Lilly.
AMS: research support from NIA-NIH and Larry L. Hillblom Foundation.
MCT: receives research funding from CIHR and NIH, and is an investigator on pharmaceutical studies with Biogen, Roche, Eli Lilly, and Boehringer.
AT: the author reports no disclosures relevant to this manuscript.
SW: receives research support from NIH.
ZKW: is partially supported by the Mayo Clinic Center for Regenerative Medicine, the gifts from The Sol Goldman Charitable Trust, and the Donald G. and Jodi P. Heeringa Family, the Haworth Family Professorship in Neurodegenerative Diseases fund, and The Albertson Parkinson’s Research Foundation. He served/s as PI or Co-PI on Abbvie, Inc. (M15-562 and M15-563), Biogen, Inc. (228PD201) grant, and Biohaven Pharmaceuticals, Inc. (BHV4157-206 and BHV3241-301). He serves as PI of the Mayo Clinic American Parkinson Disease Association (APDA) Information and Referral Center, and as Co-PI of the Mayo Clinic APDA Center for Advanced Research. He is a Co-Editor-in-Chief of the Neurologia i Neurochirurgia Polska (Polish Journal of Neurology and Neurosurgery). He is a former Co-Editor-in-Chief of Parkinsonism and Related Disorders, and former Associated Editor of the European Journal of Neurology.
BFB: research support from NIH, and research support for clinical trials sponsored by Biogen, Alector, and EIP Pharma. He serves on the Scientific Advisory Board of the Tau Consortium.
ALB: research support from NIH, the Tau Research Consortium, the Association for Frontotemporal Degeneration, Bluefield Project to Cure Frontotemporal Dementia, Corticobasal Degeneration Solutions, the Association for Frontotemporal Degeneration and the Alzheimer’s Association. He has served as a consultant for Abbvie, AGTC, Alector, Arkuda, Arvinas, Asceneuron, AZTherapeutics, Bioage, Ionis, Lundbeck, Passage BIO, Regeneron, Samumed, Transposon and UCB, and received research support from Biogen, Eisai, Eli Lilly, Genentech, Novartis, Roche and TauRx.
HJR: has received research support from Biogen Pharmaceuticals, has consulting agreements with Wave Neuroscience and Ionis Pharmaceuticals, and receives research support from NIH.
KPR: receives research funding from NIH, Quest Diagnostics, Rainwater Charitable Foundation, and Marcus Family Foundation.
Figures
References
-
- Dermody N, Wong S, Ahmed R, Piguet O, Hodges JR, Irish M. Uncovering the Neural Bases of Cognitive and Affective Empathy Deficits in Alzheimer’s Disease and the Behavioral-Variant of Frontotemporal Dementia. JAlzheimer’s Dis. 2016;(Preprint):1–16. - PubMed
Publication types
MeSH terms
Grants and funding
- K23 AG061253/AG/NIA NIH HHS/United States
- K24 AG045333/AG/NIA NIH HHS/United States
- U19 AG063911/AG/NIA NIH HHS/United States
- U01 NS080818/NS/NINDS NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- P30 AG066530/AG/NIA NIH HHS/United States
- K23 AG059888/AG/NIA NIH HHS/United States
- U01 AG045390/AG/NIA NIH HHS/United States
- U54 NS092089/NS/NINDS NIH HHS/United States
- R25 NS098999/NS/NINDS NIH HHS/United States
- P50 AG005131/AG/NIA NIH HHS/United States
- U01 NS100610/NS/NINDS NIH HHS/United States
- RF1 AG029577/AG/NIA NIH HHS/United States
- R01 AG029577/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- P20 GM109025/GM/NIGMS NIH HHS/United States
- P30 AG066509/AG/NIA NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- U01 NS090259/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
