

MYB/MYBL1::QKI fusion-positive diffuse glioma
- PMID: 36592415
- PMCID: PMC9941827
- DOI: 10.1093/jnen/nlac123
MYB/MYBL1::QKI fusion-positive diffuse glioma
Abstract
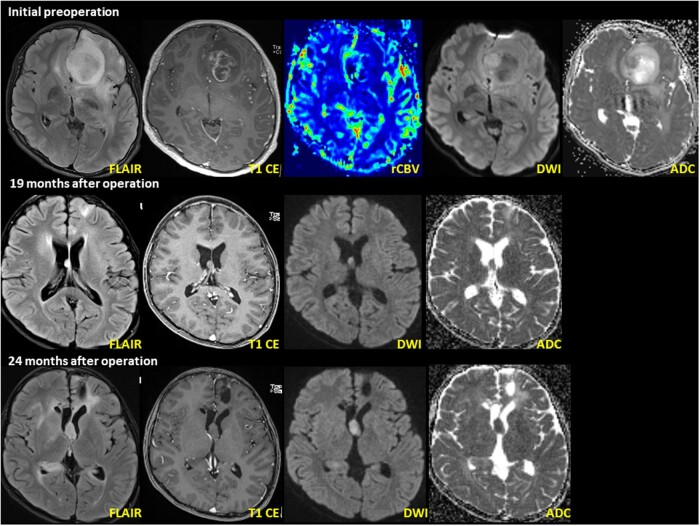
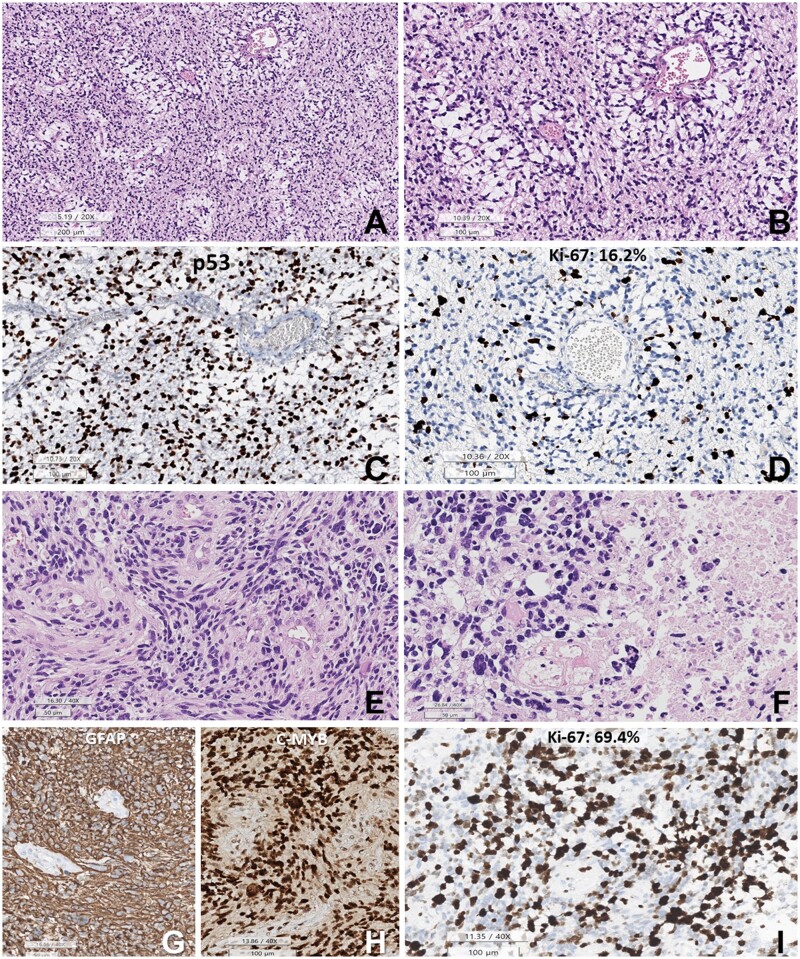
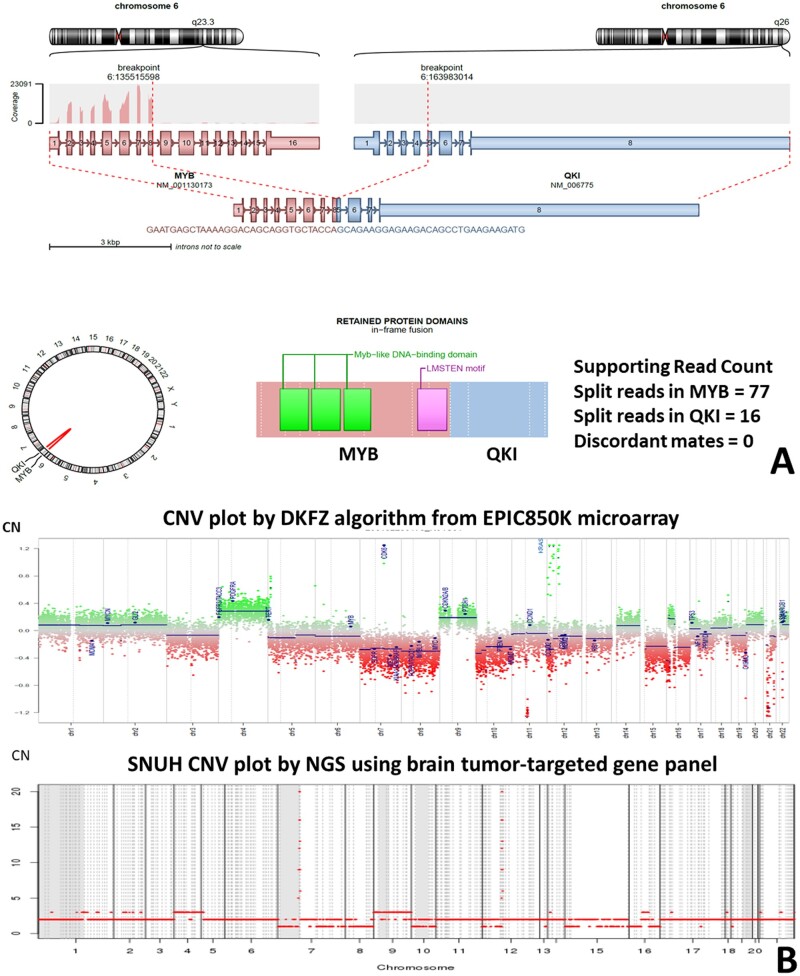
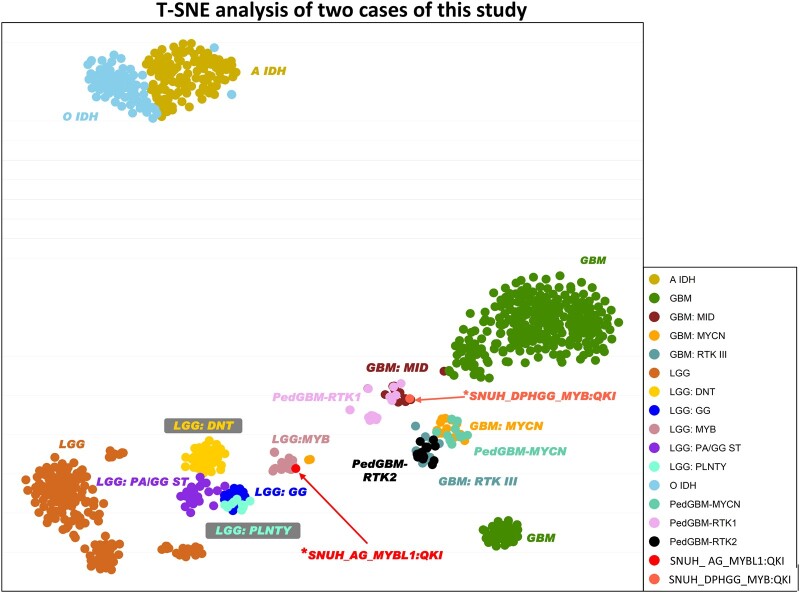
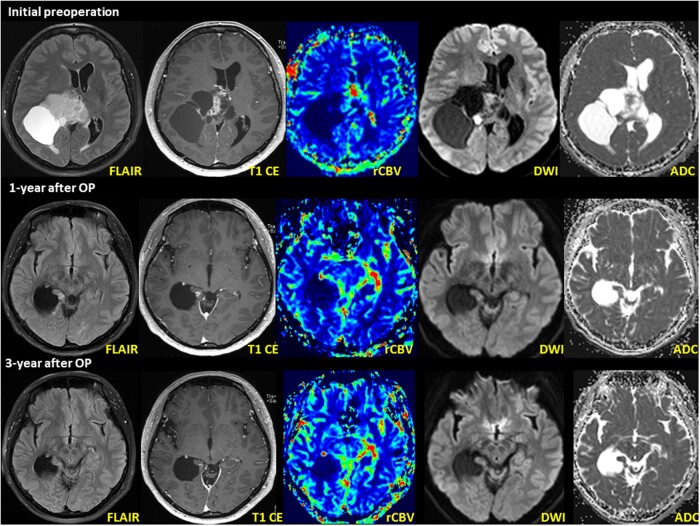
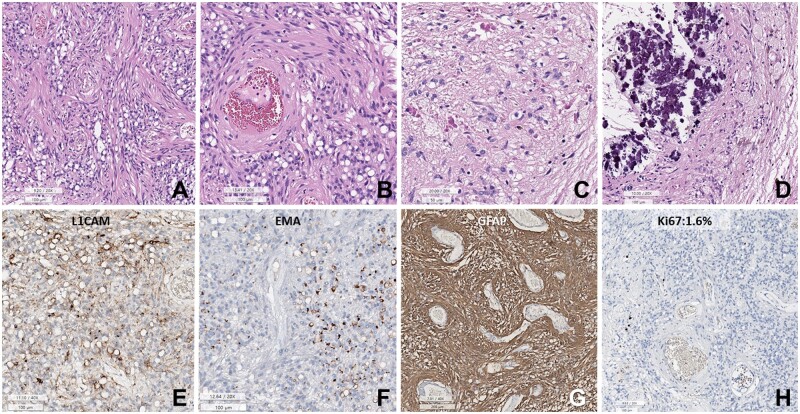
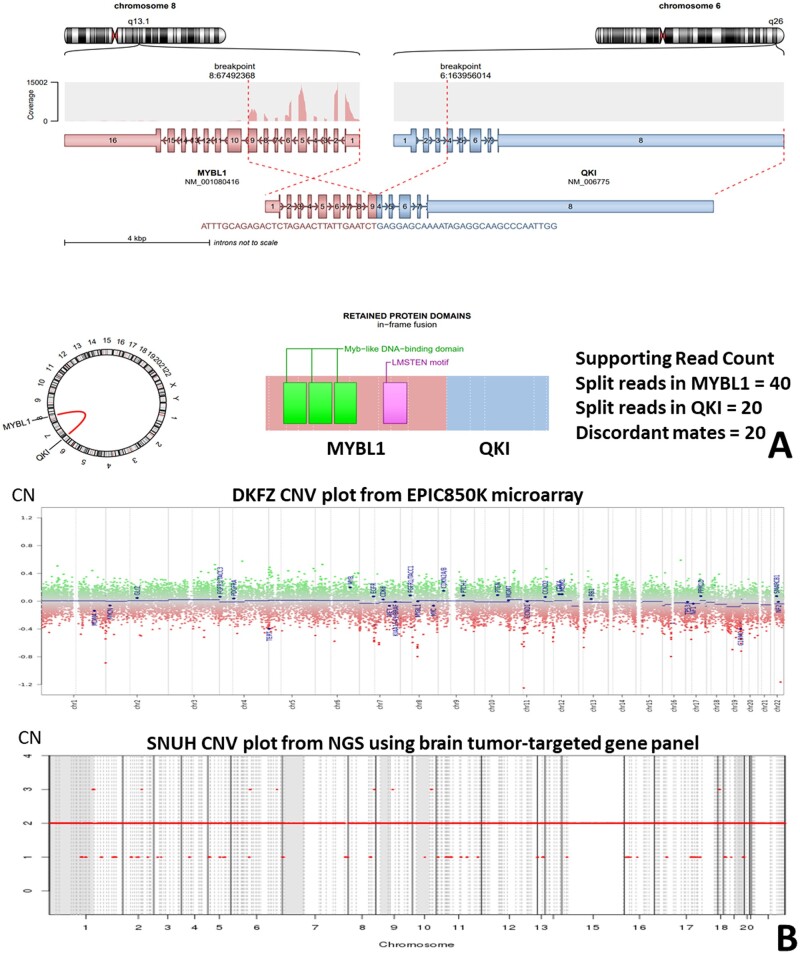
The MYB/MYBL1::QKI fusion induces the protooncogene, MYB, and deletes the tumor suppressor gene, QKI. MYB/MYBL1::QKI rearrangement was previously reported only in angiocentric glioma (AG) and diffuse low-grade glioma. This report compares 2 tumors containing the MYB/MYBL1::QKI fusion: a diffuse pediatric-type high-grade glioma (DPedHGG) in an 11-year-old boy and an AG in a 46-year-old woman. We used immunohistochemistry, next-generation sequencing, and methylation profiling to characterize each tumor and compare our findings to the literature on AG and tumors with the MYB/MYBL1::QKI rearrangement. Both tumors were astrocytic with angiocentric patterns. The MYB::QKI fusion-positive DPedHGG, which recurred once, was accompanied by TP53 mutation and amplification of CDK6 and KRAS, suggesting malignant transformation secondary to additional genetic aberrations. The second case was the adult AG with MYBL1::QKI fusion, which mimicked ependymoma based on histopathology and its dot- and ring-like epithelial membrane antigen positivity. Combined with a literature review, our results suggest that MYB/MYBL1 alterations are not limited to low-grade gliomas, including AG. AG is most common in the cerebra of children and adolescents but exceptional cases occur in adults and the acquisition of additional genetic mutations may contribute to high-grade glioma. These cases further demonstrate that molecular characteristics, morphologic features, and clinical context are essential for diagnosis.
Keywords: MYB/MYBL1-alteration; Angiocentric glioma; Methylation profile; Next-generation sequencing; Pediatric-type high-grade glioma.
© The Author(s) 2023. Published by Oxford University Press on behalf of American Association of Neuropathologists, Inc.
Figures
References
-
- Lian F, Wang LM, Qi XL, et al. MYB-QKI rearrangement in angiocentric glioma. Clin Neuropathol 2020;39:263–70 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
