

Review of Pediatric Extraosseous Chordomas with a Unique, Illustrative Case
- PMID: 36592618
- PMCID: PMC10064394
- DOI: 10.1159/000528761
Review of Pediatric Extraosseous Chordomas with a Unique, Illustrative Case
Abstract
Introduction: Chordoma is a rare, aggressive tumor that is believed to originate from notochord remnants. It can occur anywhere from the clivus to the sacrum and often recurs even after resection and radiotherapy. We present a unique case that initially suggested a different pathology based on imaging and presentation but was found to be a chordoma on gross and pathological analysis.
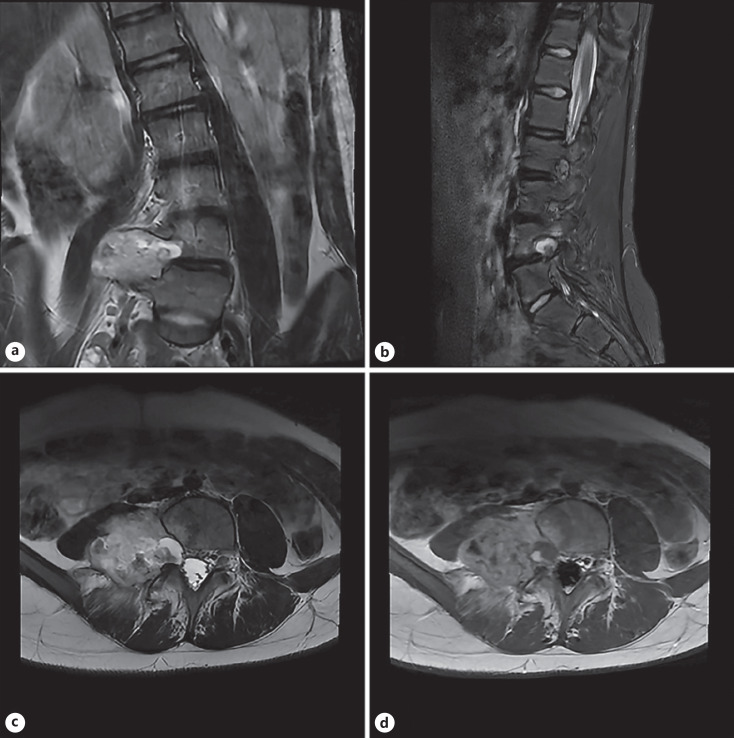
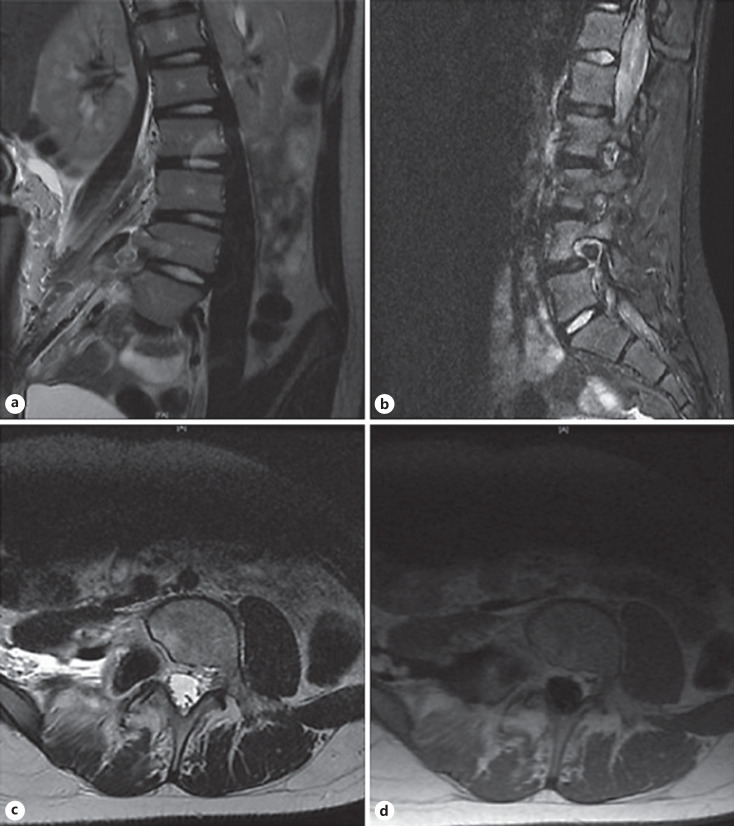
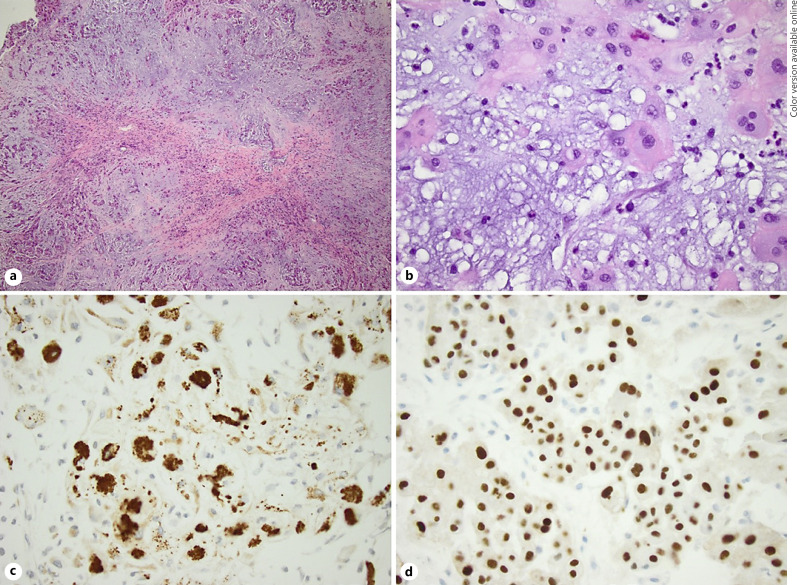
Case presentation: An 11-year-old girl presented outpatient for scoliosis evaluation and was found to have what appeared to be a right L4 peripheral nerve sheath tumor on MRI, causing dextroconvex scoliosis. She underwent a gross total resection via a retroperitoneal approach and was found to have what appeared to be an extraosseous, extradural, extra-spinal canal lumbar chordoma. Immunohistochemical features on surgical pathology were consistent with chordoma. The patient was referred to radiation oncology for adjuvant radiotherapy and pediatric hematology/oncology for recurrence monitoring.
Discussion: Our case is the first to present in such a manner, was shown to be external to the spinal canal, encasing the nerve root, and was the first such case in a pediatric patient. We reviewed the growing body of literature on spinal extraosseous chordomas and their characteristics within the pediatric patient population. We also reviewed chordoma pathogenesis theories as well as current and future treatment options.
Keywords: Extraosseous chordoma; Lumbar chordoma; Pediatric chordoma; Spinal oncology.
The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- McMaster ML, Goldstein AM, Bromley CM, Ishibe N, Parry DM. Chordoma: incidence and survival patterns in the United States, 1973–1995. Cancer Causes Control. 2001 Jan;12((1)):1–11. - PubMed
-
- Frezza AM, Botta L, Trama A, Dei Tos AP, Stacchiotti S. Chordoma: update on disease, epidemiology, biology and medical therapies. Curr Opin Oncol. 2019 Mar;31((2)):114–120. - PubMed
-
- Ridenour RV, 3rd, Ahrens WA, Folpe AL, Miller DV. Clinical and histopathologic features of chordomas in children and young adults. Pediatr Dev Pathol. 2010 Jan-Feb;13((1)):9–17. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
