

CD4 CAR-T cells targeting CD19 play a key role in exacerbating cytokine release syndrome, while maintaining long-term responses
- PMID: 36593069
- PMCID: PMC9809278
- DOI: 10.1136/jitc-2022-005878
CD4 CAR-T cells targeting CD19 play a key role in exacerbating cytokine release syndrome, while maintaining long-term responses
Abstract
Background: To date, T cells redirected with CD19-specific chimeric antigen receptors (CAR) have gained impressive success in B-cell malignancies. However, treatment failures are common and the occurrence of severe toxicities, such as cytokine release syndrome (CRS), still limits the full exploitation of this approach. Therefore, the development of cell products with improved therapeutic indexes is highly demanded.
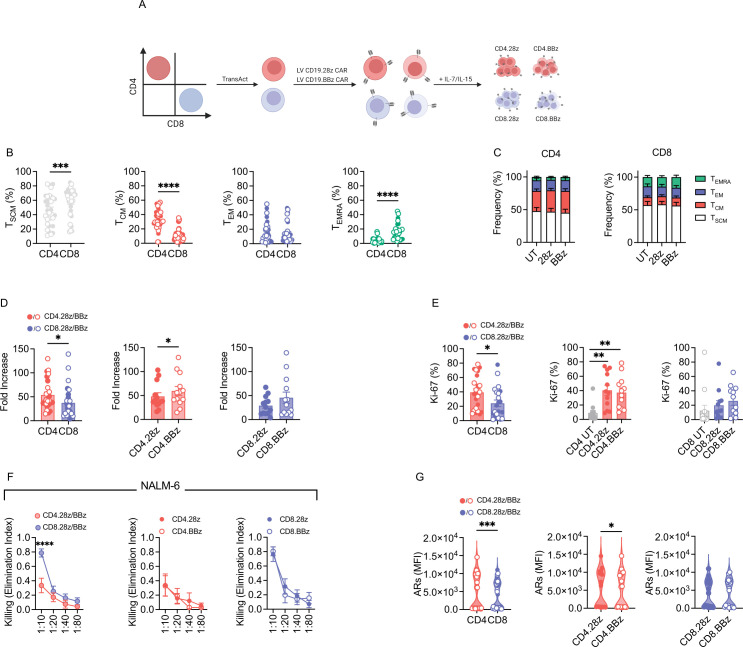
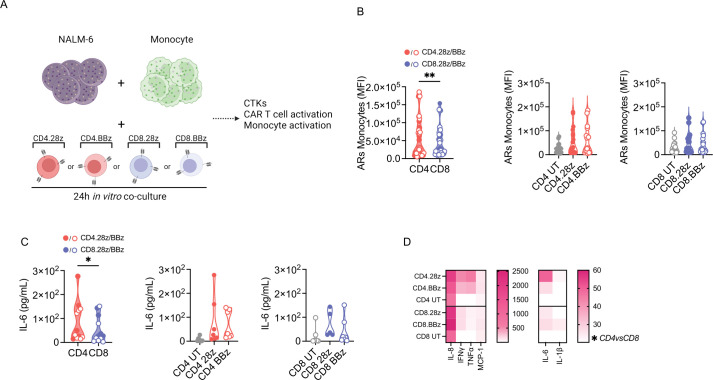
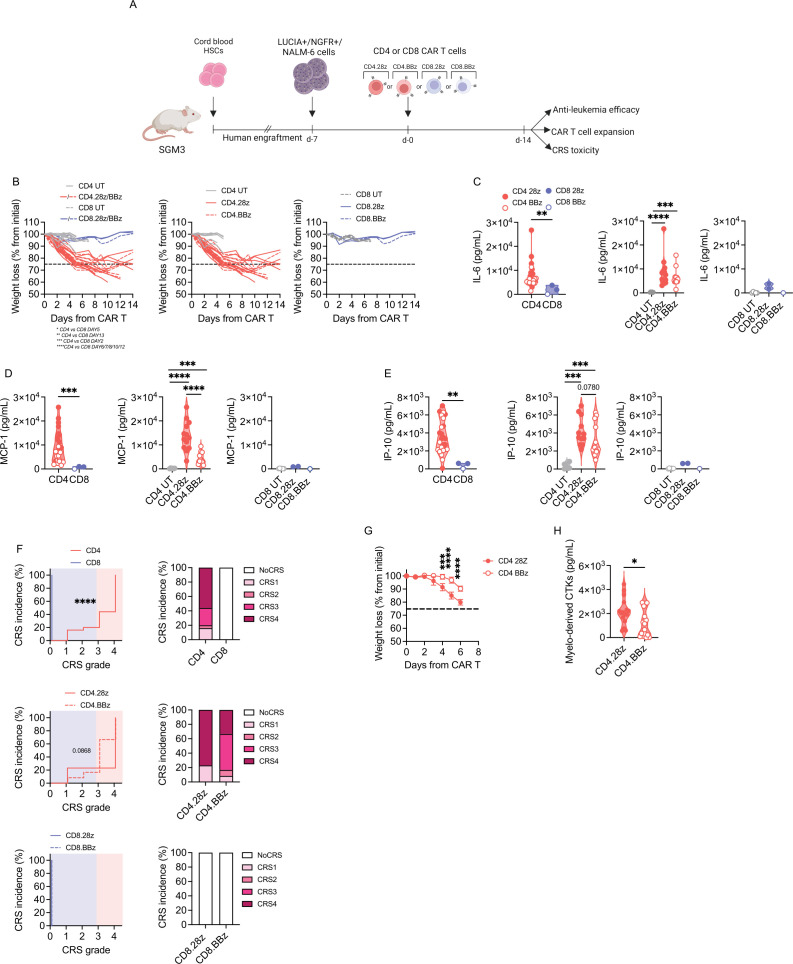
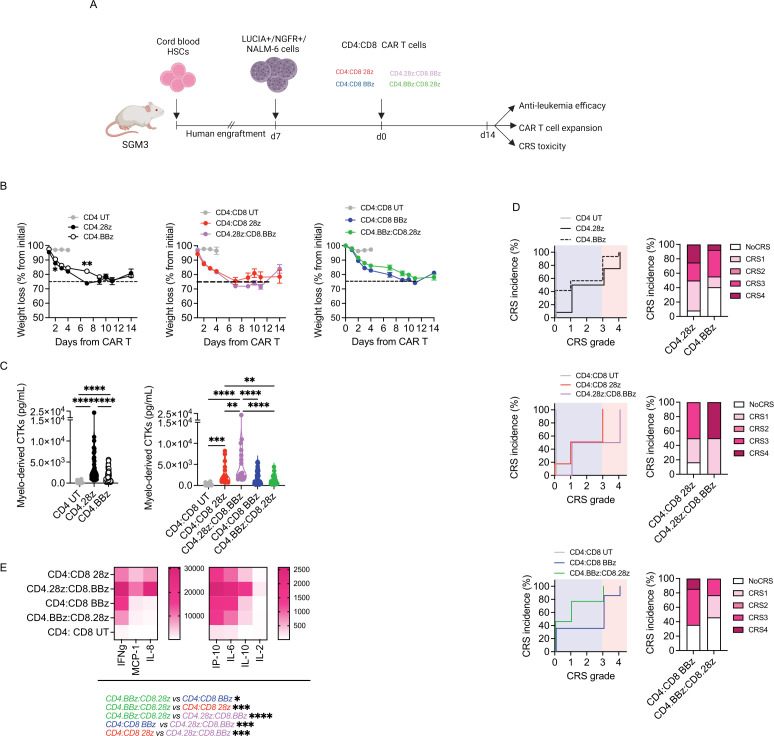
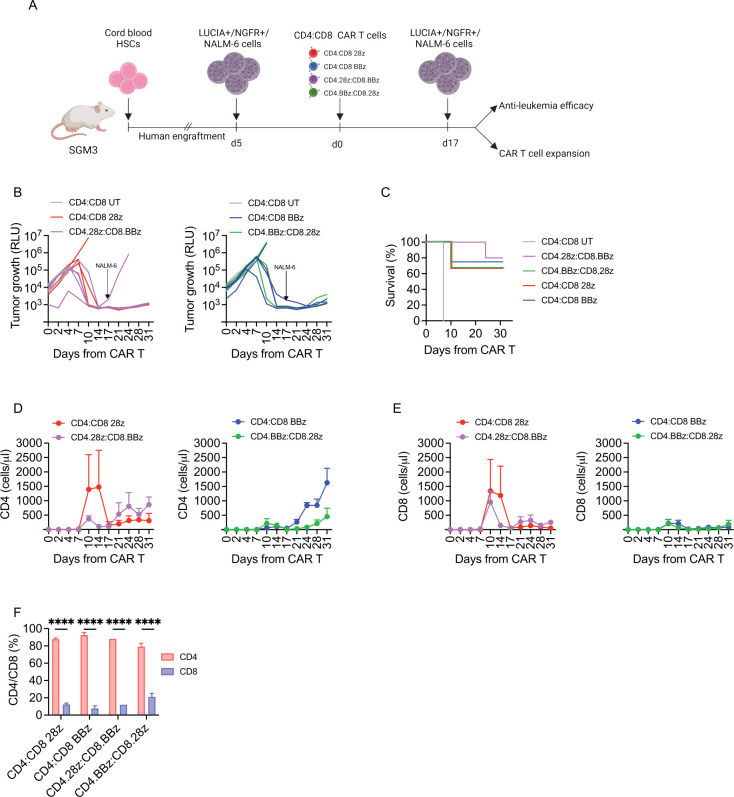
Methods: In this project, we investigated how CD4 and CD8 populations cooperate during CD19 CAR-T cell responses and what is their specific role in CRS development. To this aim, we took advantage of immunodeficient mice reconstituted with a human immune system (HuSGM3) and engrafted with the B-cell acute lymphoblastic leukemia cell line NALM-6, a model that allows to thoroughly study efficacy and toxicity profiles of CD19 CAR-T cell products.
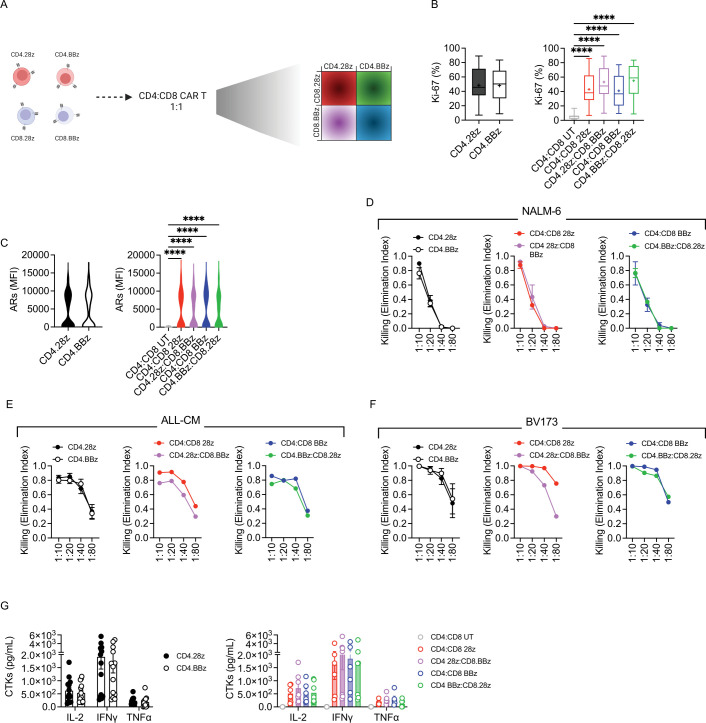
Results: CD4 CAR-T cells showed superior proliferation and activation potential, which translated into stronger stimulation of myeloid cells, the main triggers of adverse events. Accordingly, toxicity assessment in HuSGM3 mice identified CD4 CAR-T cells as key contributors to CRS development, revealing a safer profile when they harbor CARs embedded with 4-1BB, rather than CD28. By comparing differentially co-stimulated CD4:CD8 1:1 CAR-T cell formulations, we observed that CD4 cells shape the overall expansion kinetics of the infused product and are crucial for maintaining long-term responses. Interestingly, the combination of CD4.BBz with CD8.28z CAR-T cells resulted in the lowest toxicity, without impacting antitumor efficacy.
Conclusions: Taken together, these data point out that the rational design of improved adoptive T-cell therapies should consider the biological features of CD4 CAR-T cells, which emerged as crucial for maintaining long-term responses but also endowed by a higher toxic potential.
Keywords: CD4-Positive T-Lymphocytes; CD8-Positive T-Lymphocytes; Cytokines; Immunotherapy; Receptors, Chimeric Antigen.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: CBon received research support from Intellia Therapeutics. ABo is currently an employee of AstraZeneca. His contribution to this work relates to the period 2016–2017 when he was an employee of Vita-Salute San Raffaele University. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials