

Cardiorespiratory signature of neonatal sepsis: development and validation of prediction models in 3 NICUs
- PMID: 36593281
- PMCID: PMC10314957
- DOI: 10.1038/s41390-022-02444-7
Cardiorespiratory signature of neonatal sepsis: development and validation of prediction models in 3 NICUs
Abstract
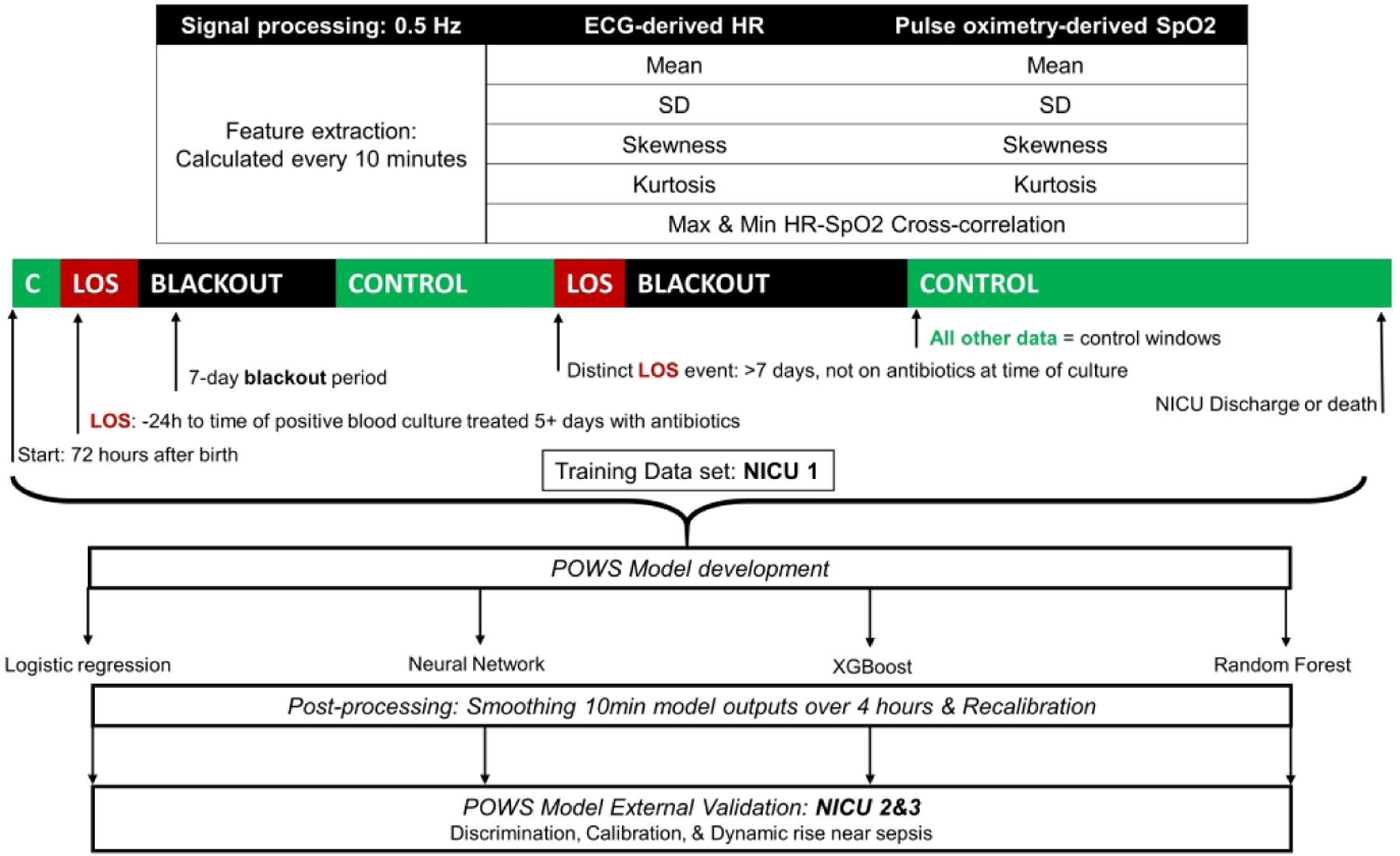
Background: Heart rate characteristics aid early detection of late-onset sepsis (LOS), but respiratory data contain additional signatures of illness due to infection. Predictive models using cardiorespiratory data may improve early sepsis detection. We hypothesized that heart rate (HR) and oxygenation (SpO2) data contain signatures that improve sepsis risk prediction over HR or demographics alone.
Methods: We analyzed cardiorespiratory data from very low birth weight (VLBW, <1500 g) infants admitted to three NICUs. We developed and externally validated four machine learning models to predict LOS using features calculated every 10 m: mean, standard deviation, skewness, kurtosis of HR and SpO2, and cross-correlation. We compared feature importance, discrimination, calibration, and dynamic prediction across models and cohorts. We built models of demographics and HR or SpO2 features alone for comparison with HR-SpO2 models.
Results: Performance, feature importance, and calibration were similar among modeling methods. All models had favorable external validation performance. The HR-SpO2 model performed better than models using either HR or SpO2 alone. Demographics improved the discrimination of all physiologic data models but dampened dynamic performance.
Conclusions: Cardiorespiratory signatures detect LOS in VLBW infants at 3 NICUs. Demographics risk-stratify, but predictive modeling with both HR and SpO2 features provides the best dynamic risk prediction.
Impact: Heart rate characteristics aid early detection of late-onset sepsis, but respiratory data contain signatures of illness due to infection. Predictive models using both heart rate and respiratory data may improve early sepsis detection. A cardiorespiratory early warning score, analyzing heart rate from electrocardiogram or pulse oximetry with SpO2, predicts late-onset sepsis within 24 h across multiple NICUs and detects sepsis better than heart rate characteristics or demographics alone. Demographics risk-stratify, but predictive modeling with both HR and SpO2 features provides the best dynamic risk prediction. The results increase understanding of physiologic signatures of neonatal sepsis.
© 2022. The Author(s), under exclusive licence to the International Pediatric Research Foundation, Inc.
Conflict of interest statement
Competing Interests statement: Some authors have financial conflicts of interest. JRM and DEL own stock in Medical Prediction Sciences Corporation. JRM is a consultant for Nihon Kohden Digital Health Solutions. ZAV is a consultant for Medtronic. All other authors have no financial conflicts to disclose. No authors have any non-financial conflicts of interest to disclose.
Figures




References
-
- King WE, Carlo WA, O’Shea TM, Schelonka RL, HRC neurodevelopmental follow-up investigators. Heart rate characteristics monitoring and reduction in mortality or neurodevelopmental impairment in extremely low birthweight infants with sepsis. Early Hum Dev 2021. Aug;159:105419. - PubMed
-
- Ting, et al. Duration of initial empirical antibiotic therapy and outcomes in very low birth weight infants. Pediatrics 2019. Mar;143(3). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
