

Flexible treatment of gestational diabetes mellitus adjusted according to intrauterine fetal growth versus treatment according to strict maternal glycemic parameters: a randomized clinical trial
- PMID: 36593648
- PMCID: PMC9730386
- DOI: 10.1136/bmjdrc-2022-002915
Flexible treatment of gestational diabetes mellitus adjusted according to intrauterine fetal growth versus treatment according to strict maternal glycemic parameters: a randomized clinical trial
Abstract
Introduction: To compare the conventional treatment of gestational diabetes mellitus (GDM) with flexible treatment according to the measurement of fetal abdominal circumference (AC) in daily clinical practice.
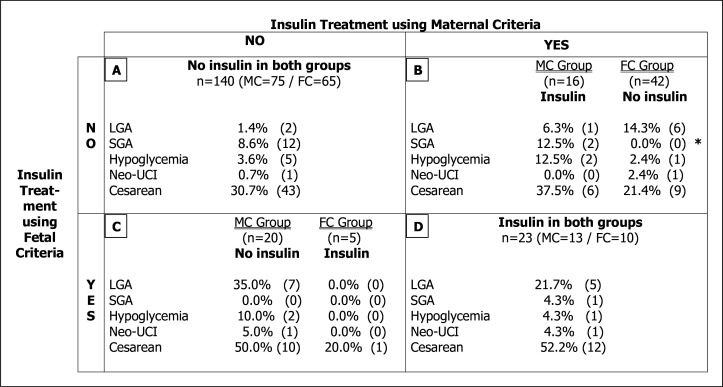
Research design and methods: Two hundred and sixty pregnant women diagnosed with GDM before week 34 were randomly placed in two groups: a control group, treated according to maternal capillary glycemia, and an experimental group, treated according to ultrasound parameters of fetal growth. The glycemic targets in the control group were blood glucose levels when fasting and 1 hour postprandial (<95/140 mg/dL). In the experimental group, glycemic targets depended on the percentile (p) of fetal AC: if AC p <75th, then blood glucose targets when fasting and at 1 hour postprandial were <120/180 mg/dL; and if AC p ≥75th, then the glycemic targets were <80/120 mg/dL. The follow-up of both groups was scheduled according to the GDM protocol of our diabetes and gestation unit.
Results: The study was completed by 246 pregnant women, 125 in the control group and 121 in the experimental group. In the experimental group, insulin treatment and neonatal hypoglycemia were significantly lower (p=0.018 and p 0.035, respectively). No differences were observed in large and small infants according to gestational age. However, macrosomic infants were less frequent in the experimental group, although this difference did not reach statistical significance. In terms of gestation complications, the type of delivery and its complications and the rest of the neonatal complications analyzed, no significant differences were observed.
Conclusions: The treatment of flexible GDM according to the measurement of fetal AC is safe for the mother and the fetus and almost halves the number of pregnant women who require insulin treatment, without increasing the number of ultrasound checks or medical visits.
Keywords: Birth Weight; Gestational Diabetes Mellitus; Insulin; Ultrasonography.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
A randomized controlled trial using glycemic plus fetal ultrasound parameters versus glycemic parameters to determine insulin therapy in gestational diabetes with fasting hyperglycemia.Diabetes Care. 2001 Nov;24(11):1904-10. doi: 10.2337/diacare.24.11.1904. Diabetes Care. 2001. PMID: 11679455 Clinical Trial.
-
A randomized trial evaluating a predominantly fetal growth-based strategy to guide management of gestational diabetes in Caucasian women.Diabetes Care. 2004 Feb;27(2):297-302. doi: 10.2337/diacare.27.2.297. Diabetes Care. 2004. PMID: 14747203 Clinical Trial.
-
Use of fetal ultrasound to select metabolic therapy for pregnancies complicated by mild gestational diabetes.Diabetes Care. 1994 Apr;17(4):275-83. doi: 10.2337/diacare.17.4.275. Diabetes Care. 1994. PMID: 8026282 Clinical Trial.
-
Gestational diabetes mellitus management according to ultrasound fetal growth versus strict glycemic treatment in singleton pregnancies: A systematic review and meta-analysis of clinical trials.J Obstet Gynaecol Res. 2024 Oct;50(10):1759-1770. doi: 10.1111/jog.16059. Epub 2024 Aug 25. J Obstet Gynaecol Res. 2024. PMID: 39183485
-
Screening and diagnosing gestational diabetes mellitus.Evid Rep Technol Assess (Full Rep). 2012 Oct;(210):1-327. Evid Rep Technol Assess (Full Rep). 2012. PMID: 24423035 Free PMC article. Review.
Cited by
-
Sample size calculation in clinical research.Perspect Clin Res. 2024 Jul-Sep;15(3):155-159. doi: 10.4103/picr.picr_100_24. Epub 2024 Jul 4. Perspect Clin Res. 2024. PMID: 39140012 Free PMC article.
References
-
- Crowther CA, Hiller JE, Moss JR. Australian carbohydrate intolerance study in pregnant women (ACHOIS) trial Group. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med 2005;352:2477–86. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical