

Effect of Remifentanil vs Neuromuscular Blockers During Rapid Sequence Intubation on Successful Intubation Without Major Complications Among Patients at Risk of Aspiration: A Randomized Clinical Trial
- PMID: 36594947
- PMCID: PMC9856823
- DOI: 10.1001/jama.2022.23550
Effect of Remifentanil vs Neuromuscular Blockers During Rapid Sequence Intubation on Successful Intubation Without Major Complications Among Patients at Risk of Aspiration: A Randomized Clinical Trial
Erratum in
-
Incorrect Units of Measure in a Table.JAMA. 2023 Feb 14;329(6):515. doi: 10.1001/jama.2023.0424. JAMA. 2023. PMID: 36786804 Free PMC article. No abstract available.
Abstract
Importance: It is uncertain whether a rapid-onset opioid is noninferior to a rapid-onset neuromuscular blocker during rapid sequence intubation when used in conjunction with a hypnotic agent.
Objective: To determine whether remifentanil is noninferior to rapid-onset neuromuscular blockers for rapid sequence intubation.
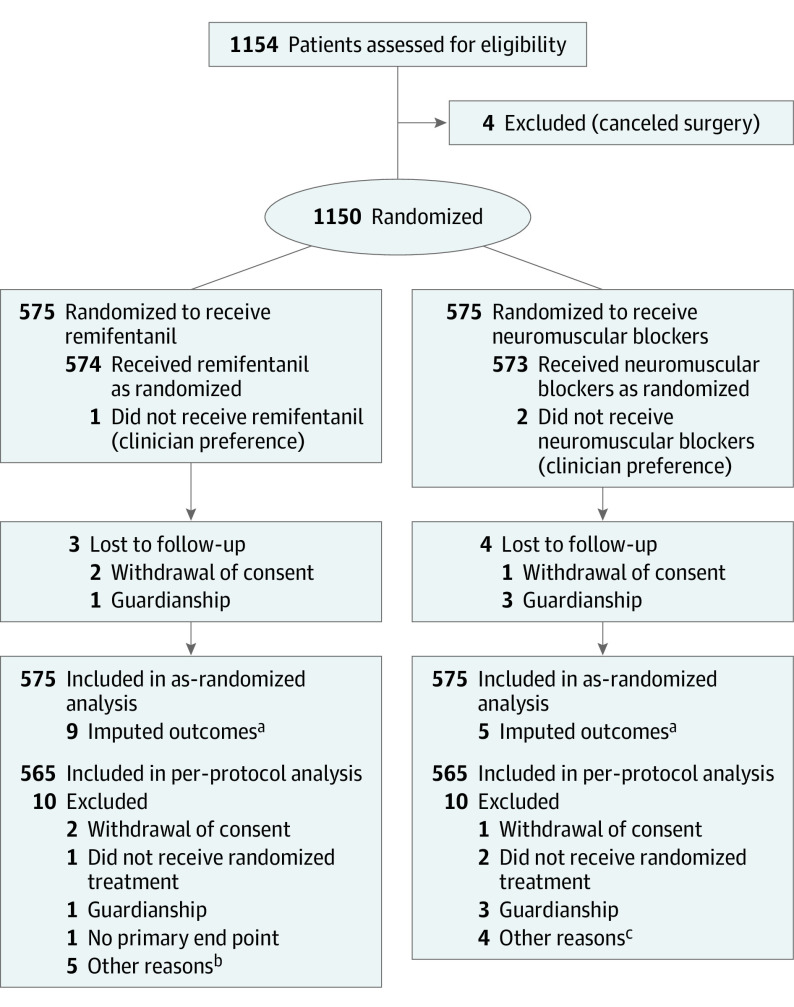
Design, setting, and participants: Multicenter, randomized, open-label, noninferiority trial among 1150 adults at risk of aspiration (fasting for <6 hours, bowel occlusion, recent trauma, or severe gastroesophageal reflux) who underwent tracheal intubation in the operating room at 15 hospitals in France from October 2019 to April 2021. Follow-up was completed on May 15, 2021.
Interventions: Patients were randomized to receive neuromuscular blockers (1 mg/kg of succinylcholine or rocuronium; n = 575) or remifentanil (3 to 4 μg/kg; n = 575) immediately after injection of a hypnotic.
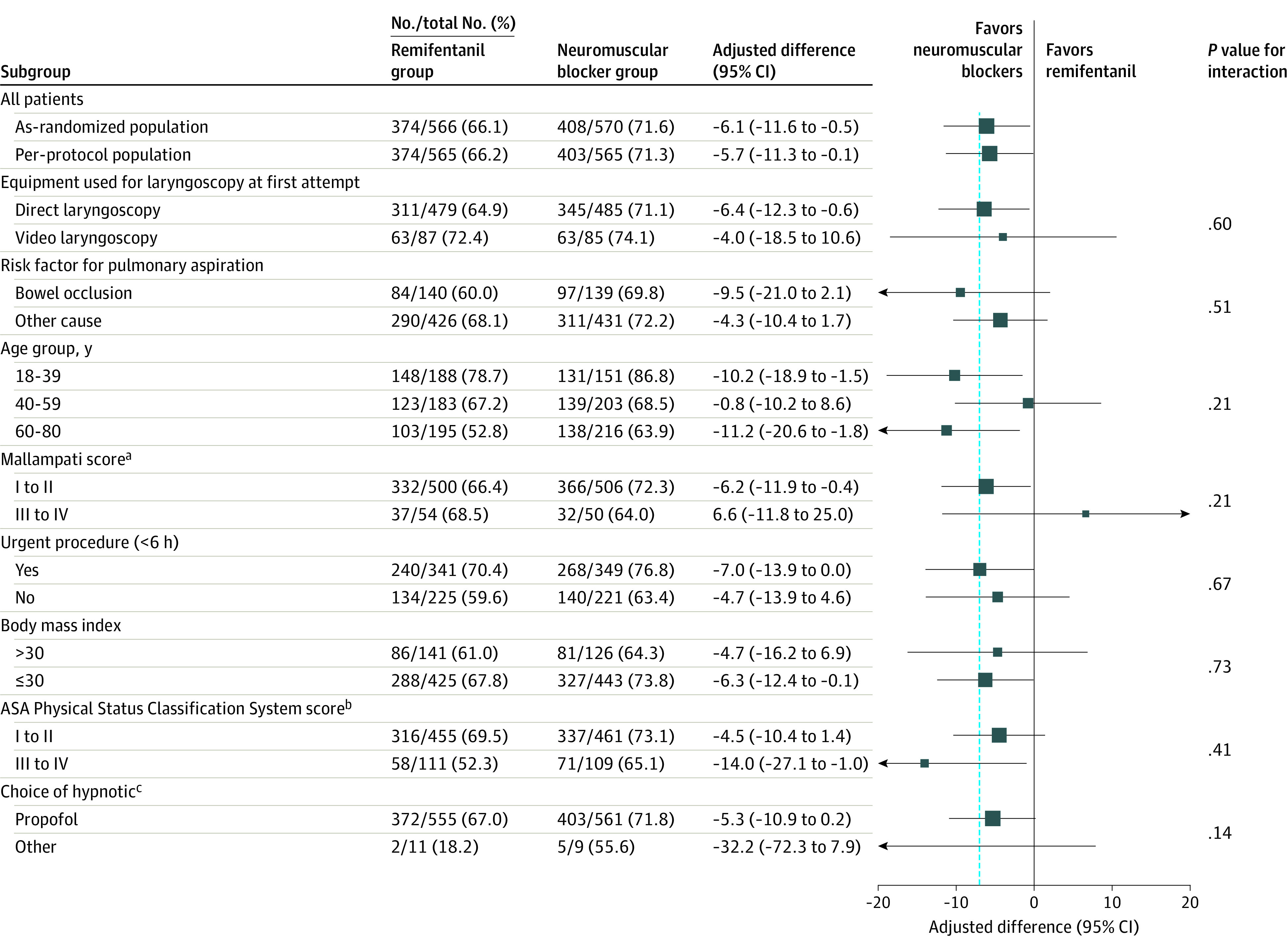
Main outcomes and measures: The primary outcome was assessed in all randomized patients (as-randomized population) and in all eligible patients who received assigned treatment (per-protocol population). The primary outcome was successful tracheal intubation on the first attempt without major complications, defined as lung aspiration of digestive content, oxygen desaturation, major hemodynamic instability, sustained arrhythmia, cardiac arrest, and severe anaphylactic reaction. The prespecified noninferiority margin was 7.0%.
Results: Among 1150 randomized patients (mean age, 50.7 [SD, 17.4] years; 573 [50%] women), 1130 (98.3%) completed the trial. In the as-randomized population, tracheal intubation on the first attempt without major complications occurred in 374 of 575 patients (66.1%) in the remifentanil group and 408 of 575 (71.6%) in the neuromuscular blocker group (between-group difference adjusted for randomization strata and center, -6.1%; 95% CI, -11.6% to -0.5%; P = .37 for noninferiority), demonstrating inferiority. In the per-protocol population, 374 of 565 patients (66.2%) in the remifentanil group and 403 of 565 (71.3%) in the neuromuscular blocker group had successful intubation without major complications (adjusted difference, -5.7%; 2-sided 95% CI, -11.3% to -0.1%; P = .32 for noninferiority). An adverse event of hemodynamic instability was recorded in 19 of 575 patients (3.3%) with remifentanil and 3 of 575 (0.5%) with neuromuscular blockers (adjusted difference, 2.8%; 95% CI, 1.2%-4.4%).
Conclusions and relevance: Among adults at risk of aspiration during rapid sequence intubation in the operating room, remifentanil, compared with neuromuscular blockers, did not meet the criterion for noninferiority with regard to successful intubation on first attempt without major complications. Although remifentanil was statistically inferior to neuromuscular blockers, the wide confidence interval around the effect estimate remains compatible with noninferiority and limits conclusions about the clinical relevance of the difference.
Trial registration: ClinicalTrials.gov Identifier: NCT03960801.
Conflict of interest statement
Figures
Comment in
-
Remifentanil vs Neuromuscular Blockers During Rapid Sequence Intubation Among Patients at Risk of Aspiration.JAMA. 2023 May 2;329(17):1517. doi: 10.1001/jama.2023.3494. JAMA. 2023. PMID: 37129659 No abstract available.
-
Remifentanil vs Neuromuscular Blockers During Rapid Sequence Intubation Among Patients at Risk of Aspiration.JAMA. 2023 May 2;329(17):1517-1518. doi: 10.1001/jama.2023.3491. JAMA. 2023. PMID: 37129660 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
