

ESR1 gene amplification and MAP3K mutations are selected during adjuvant endocrine therapies in relapsing Hormone Receptor-positive, HER2-negative breast cancer (HR+ HER2- BC)
- PMID: 36595552
- PMCID: PMC9839248
- DOI: 10.1371/journal.pgen.1010563
ESR1 gene amplification and MAP3K mutations are selected during adjuvant endocrine therapies in relapsing Hormone Receptor-positive, HER2-negative breast cancer (HR+ HER2- BC)
Abstract
Background: Previous studies have provided a comprehensive picture of genomic alterations in primary and metastatic Hormone Receptor (HR)-positive, Human Epidermal growth factor Receptor 2 (HER2)-negative breast cancer (HR+ HER2- BC). However, the evolution of the genomic landscape of HR+ HER2- BC during adjuvant endocrine therapies (ETs) remains poorly investigated.
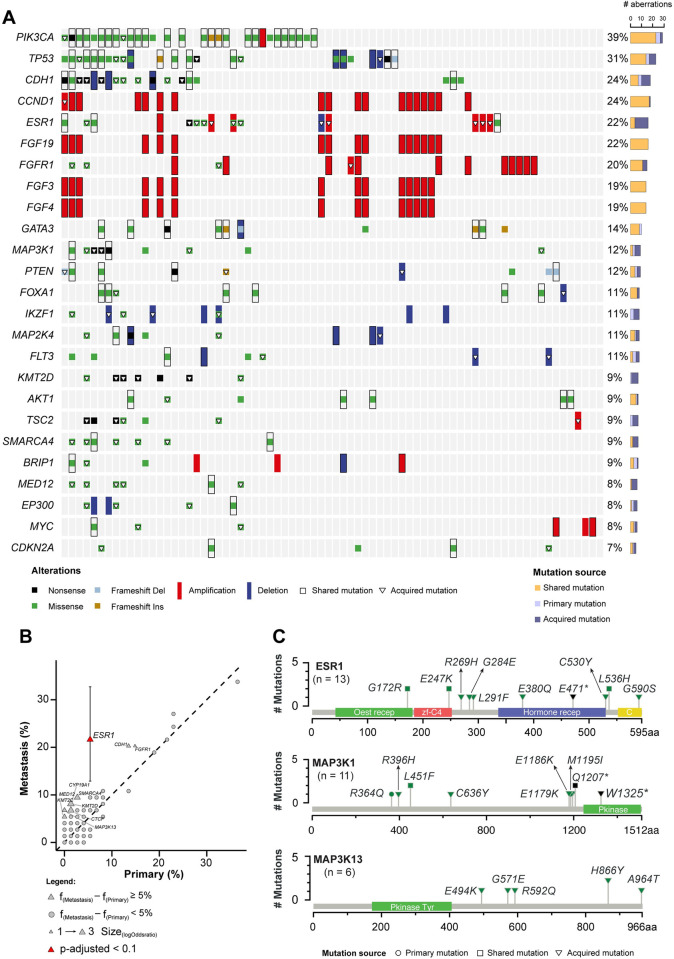
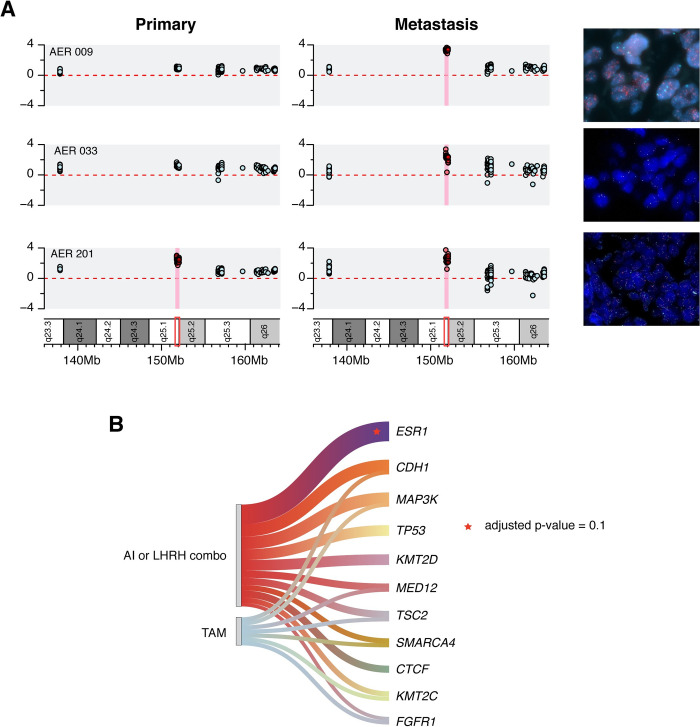
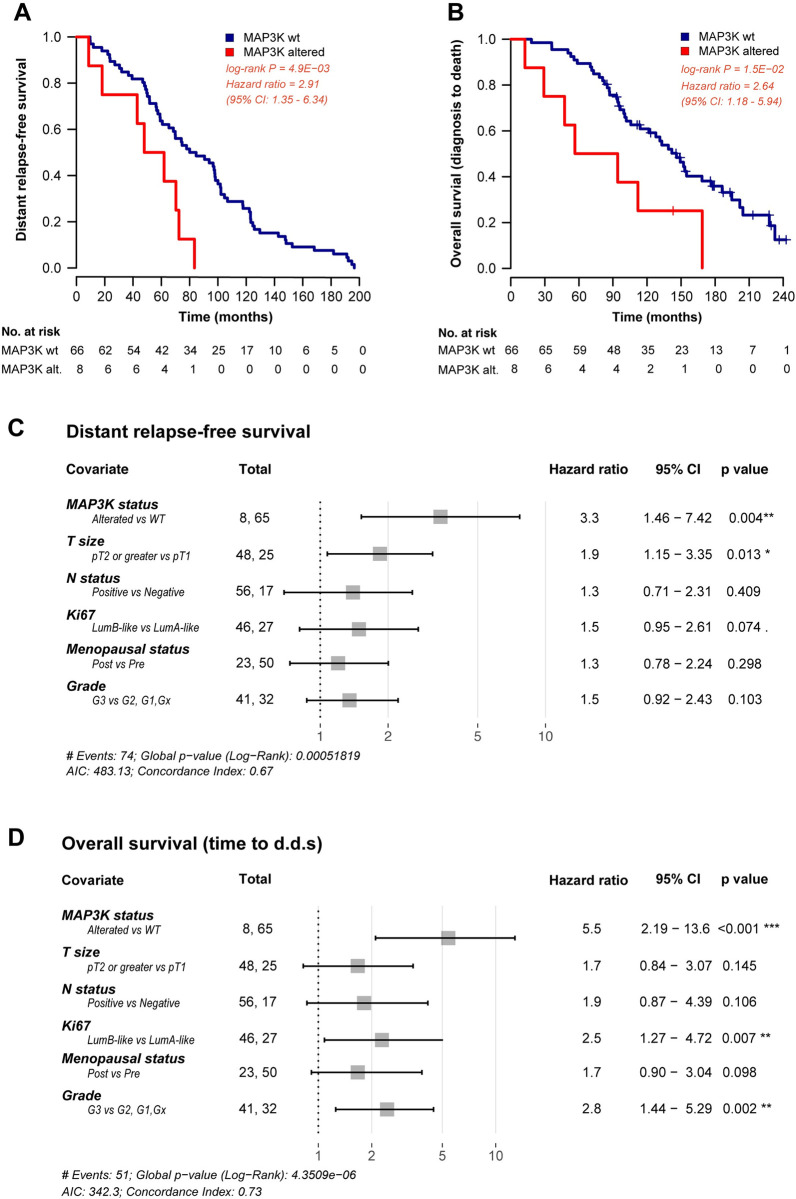
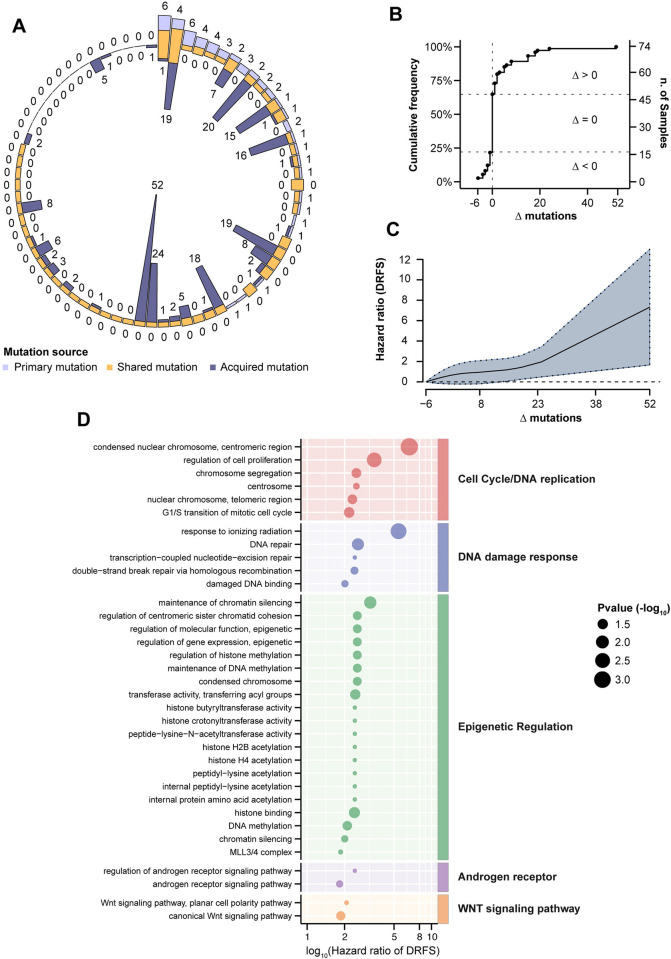
Methods and findings: We performed a genomic characterization of surgically resected HR+ HER2- BC patients relapsing during or at the completion of adjuvant ET. Using a customized panel, we comprehensively evaluated gene mutations and copy number variation (CNV) in paired primary and metastatic specimens. After retrieval and quality/quantity check of tumor specimens from an original cohort of 204 cases, 74 matched tumor samples were successfully evaluated for DNA mutations and CNV analysis. Along with previously reported genomic alterations, including PIK3CA, TP53, CDH1, GATA3 and ESR1 mutations/deletions, we found that ESR1 gene amplification (confirmed by FISH) and MAP3K mutations were enriched in metastatic lesions as compared to matched primary tumors. These alterations were exclusively found in patients treated with adjuvant aromatase inhibitors or LHRH analogs plus tamoxifen, but not in patients treated with tamoxifen alone. Patients with tumors bearing MAP3K mutations in metastatic lesions had significantly worse distant relapse-free survival (hazard ratio [HR] 3.4, 95% CI 1.52-7.70, p value 0.003) and worse overall survival (HR 5.2, 95% CI 2.10-12.8, p-value < 0.001) independently of other clinically relevant patient- and tumor-related variables.
Conclusions: ESR1 amplification and activating MAP3K mutations are potential drivers of acquired resistance to adjuvant ETs employing estrogen deprivation in HR+ HER2- BC. MAP3K mutations are associated with worse prognosis in patients with metastatic disease.
Copyright: © 2023 Ferrando et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Giancarlo Pruneri reports honoraria from Novartis, Roche, Lilly and Exact Science. Gabriele Zoppoli reports travel grants from Novartis and Pfizer, and reagents for research from Citiva and ThermoFisher Scientific. Andrea Vingiani reports honoraria from Roche and Lilly. Marco Colleoni reports Research Grant from Roche. Elisabtta Munzone reports travel grants from Roche, Pfizer, Lilly and Novartis and reports receiving consultancy fees from Eisai, Exact Sciences, MSD Oncology, Daiichi Sankyo/Astra Zeneca, Pfizer and Seagen. Giuseppe Viale has received grants from Roche/Genentech and Astra Zeneca for his institution; consulting fees from Roche/Genentech, Astra Zeneca, MDS Oncology and Daiichi Sanyko; honoraria for lectures from Roche/Genentech, Astra Zeneca and Daiichi Sanyko; support for attending meetings from Roche/Genentech; and has served on Advisory Boards for Roche/Genentech, Astra Zeneca, Pfizer, MDS Oncology and Novartis. Lorenzo Ferrando, Anna Garuti, Claudio Vernieri, Antonino Belfiore, Luca Agnelli, Gianpaolo Dagrada, Diana Ivanoiu, Giuseppina Bonizzi, Luana Lippolis, Martina Dameri, Francesco Ravera, Luca Magnani and Alberto Ballestrero have no conflict of interest to disclose.
Figures
References
-
- Aftimos P, Oliveira M, Irrthum A, Fumagalli D, Sotiriou C, Gal-Yam EN, et al. Genomic and Transcriptomic Analyses of Breast Cancer Primaries and Matched Metastases in AURORA, the Breast International Group (BIG) Molecular Screening Initiative. Cancer Discov. 2021. Nov;11(11):2796–811. doi: 10.1158/2159-8290.CD-20-1647 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
