

Sensory change and recovery of infraorbital area after zygomaticomaxillary and orbital floor fractures
- PMID: 36596749
- PMCID: PMC9816633
- DOI: 10.7181/acfs.2022.01011
Sensory change and recovery of infraorbital area after zygomaticomaxillary and orbital floor fractures
Abstract
Background: To compare the sensory change and recovery of infraorbital area associated with zygomaticomaxillary and orbital floor fractures and their recoveries and investigate the factors that affect them.
Methods: We retrospectively reviewed 652 patients diagnosed with zygomaticomaxillary (n= 430) or orbital floor (n= 222) fractures in a single center between January 2016 and January 2021. Patient data, including age, sex, medical history, injury mechanism, Knight and North classification (in zygomaticomaxillary fracture cases), injury indication for surgery (in orbital floor cases), combined injury, sensory change, and recovery period, were reviewed. The chi-square test was used for statistical analysis.
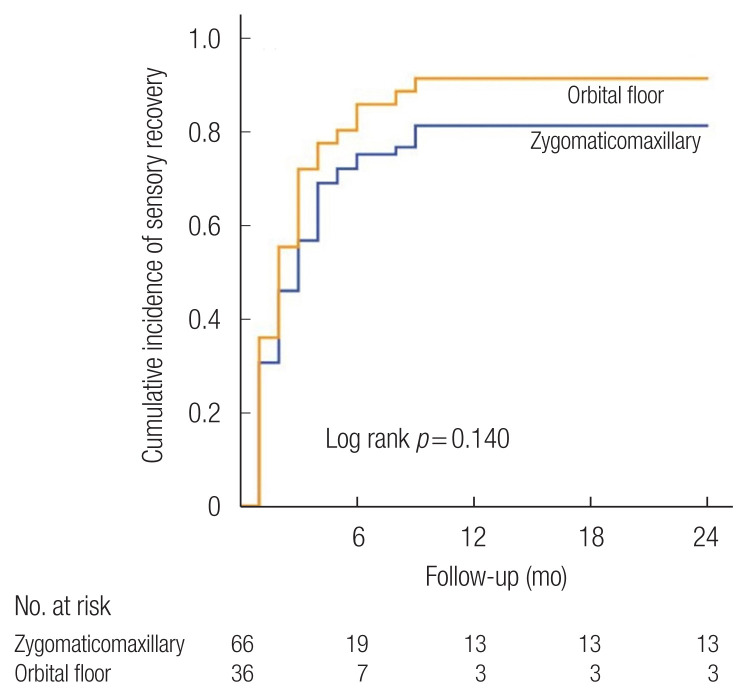
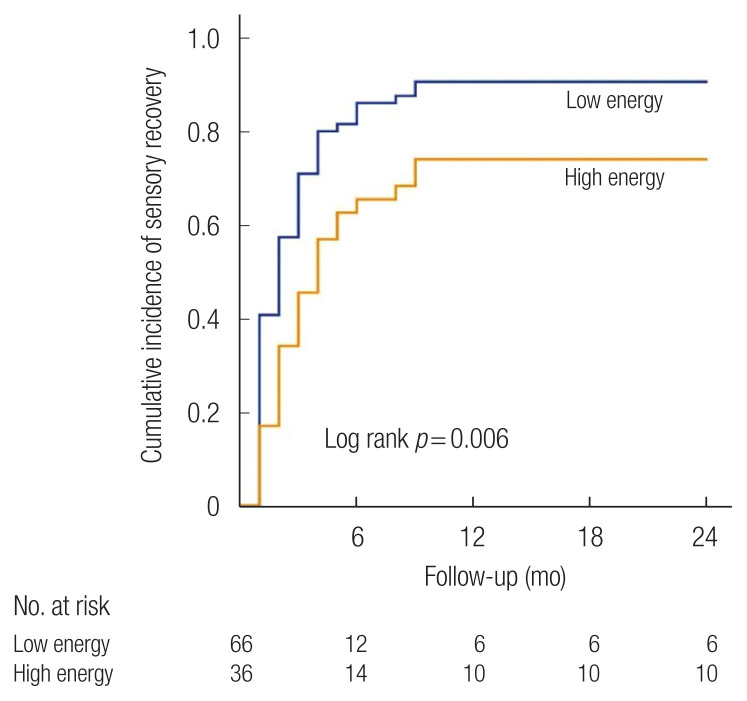
Results: Orbital floor fractures occurred more frequently in younger patients than zygomaticomaxillary fractures (p< 0.001). High-energy injuries were more likely to be associated with zygomaticomaxillary fractures (p< 0.001), whereas low-energy injuries were more likely to be associated with orbital floor fractures (p< 0.001). The sensory changes associated with orbital floor and zygomaticomaxillary fractures were not significantly different (p= 0.773). Sensory recovery was more rapid and better after orbital floor than after zygomaticomaxillary fractures; however, the difference was not significantly different. Additionally, the low-energy group showed a higher incidence of sensory changes than the high-energy group, but the difference was not statistically significant (p= 0.512). Permanent sensory changes were more frequent in the high-energy group, the difference was statistically significant (p= 0.043).
Conclusion: The study found no significant difference in the incidence of sensory changes associated with orbital floor and zygomaticomaxillary fractures. In case of orbital floor fractures and high-energy injuries, the risk of permanent sensory impairment should be considered.
Keywords: Maxillary fractures; Orbital fractures; Zygoma; Zygomatic fractures.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Kearney AM, Shah N, Zins J, Gosain AK. Fifteen-year review of the American Board of Plastic Surgery maintenance of certification tracer data: clinical practice patterns and evidence-based medicine in zygomatico-orbital fractures. Plast Reconstr Surg. 2021;147:967e–975e. - PubMed
-
- Sargent LA, Fernandez JG. Incidence and management of zygomatic fractures at a level I trauma center. Ann Plast Surg. 2012;68:472–6. - PubMed
-
- Nordgaard JO. Persistent sensory disturbances and diplopia following fractures of the zygoma. Arch Otolaryngol. 1976;102:80–2. - PubMed
-
- Hollier LH, Thornton J, Pazmino P, Stal S. The management of orbitozygomatic fractures. Plast Reconstr Surg. 2003;111:2386–92. - PubMed
-
- Homer N, Glass LR, Lee NG, Lefebvre DR, Sutula FC, Freitag SK, et al. Assessment of infraorbital hypesthesia following orbital floor and zygomaticomaxillary complex fractures using a novel sensory grading system. Ophthalmic Plast Reconstr Surg. 2019;35:53–5. - PubMed
LinkOut - more resources
Full Text Sources
