

MIMIC-IV, a freely accessible electronic health record dataset
- PMID: 36596836
- PMCID: PMC9810617
- DOI: 10.1038/s41597-022-01899-x
MIMIC-IV, a freely accessible electronic health record dataset
Erratum in
-
Author Correction: MIMIC-IV, a freely accessible electronic health record dataset.Sci Data. 2023 Jan 16;10(1):31. doi: 10.1038/s41597-023-01945-2. Sci Data. 2023. PMID: 36646711 Free PMC article. No abstract available.
-
Author Correction: MIMIC-IV, a freely accessible electronic health record dataset.Sci Data. 2023 Apr 18;10(1):219. doi: 10.1038/s41597-023-02136-9. Sci Data. 2023. PMID: 37072428 Free PMC article. No abstract available.
Abstract
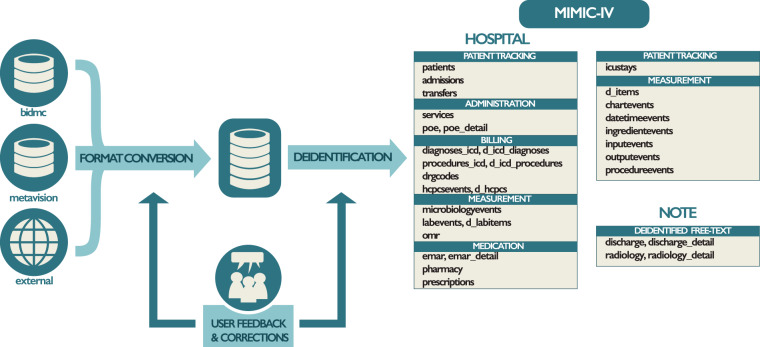
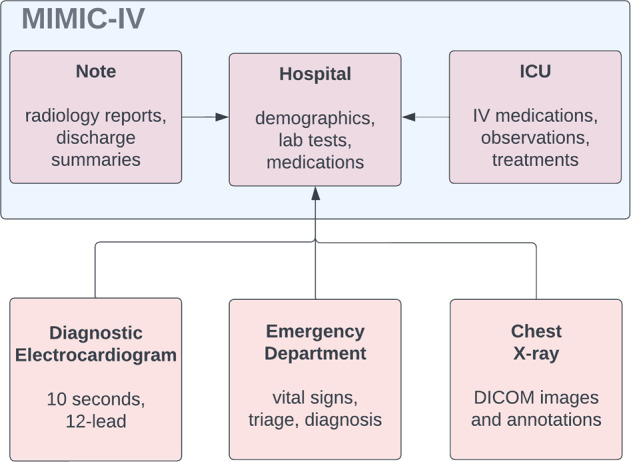
Digital data collection during routine clinical practice is now ubiquitous within hospitals. The data contains valuable information on the care of patients and their response to treatments, offering exciting opportunities for research. Typically, data are stored within archival systems that are not intended to support research. These systems are often inaccessible to researchers and structured for optimal storage, rather than interpretability and analysis. Here we present MIMIC-IV, a publicly available database sourced from the electronic health record of the Beth Israel Deaconess Medical Center. Information available includes patient measurements, orders, diagnoses, procedures, treatments, and deidentified free-text clinical notes. MIMIC-IV is intended to support a wide array of research studies and educational material, helping to reduce barriers to conducting clinical research.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Moody, G. B. & Mark, R. G. A database to support development and evaluation of intelligent intensive care monitoring. In Computers in Cardiology 1996, 657–660 (IEEE, 1996).
-
- Thoral PJ, et al. Sharing ICU patient data responsibly under the society of critical care medicine/european society of intensive care medicine joint data science collaboration: the amsterdam university medical centers database (AmsterdamUMCdb) example. Critical care medicine. 2021;49:e563. doi: 10.1097/CCM.0000000000004916. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
