

Effects of frailty, geriatric syndromes, and comorbidity on mortality and quality of life in older adults with HIV
- PMID: 36597036
- PMCID: PMC9809005
- DOI: 10.1186/s12877-022-03719-8
Effects of frailty, geriatric syndromes, and comorbidity on mortality and quality of life in older adults with HIV
Abstract
Background: To understand the effects of frailty, geriatric syndromes, and comorbidity on quality of life and mortality in older adults with HIV (OAWH).
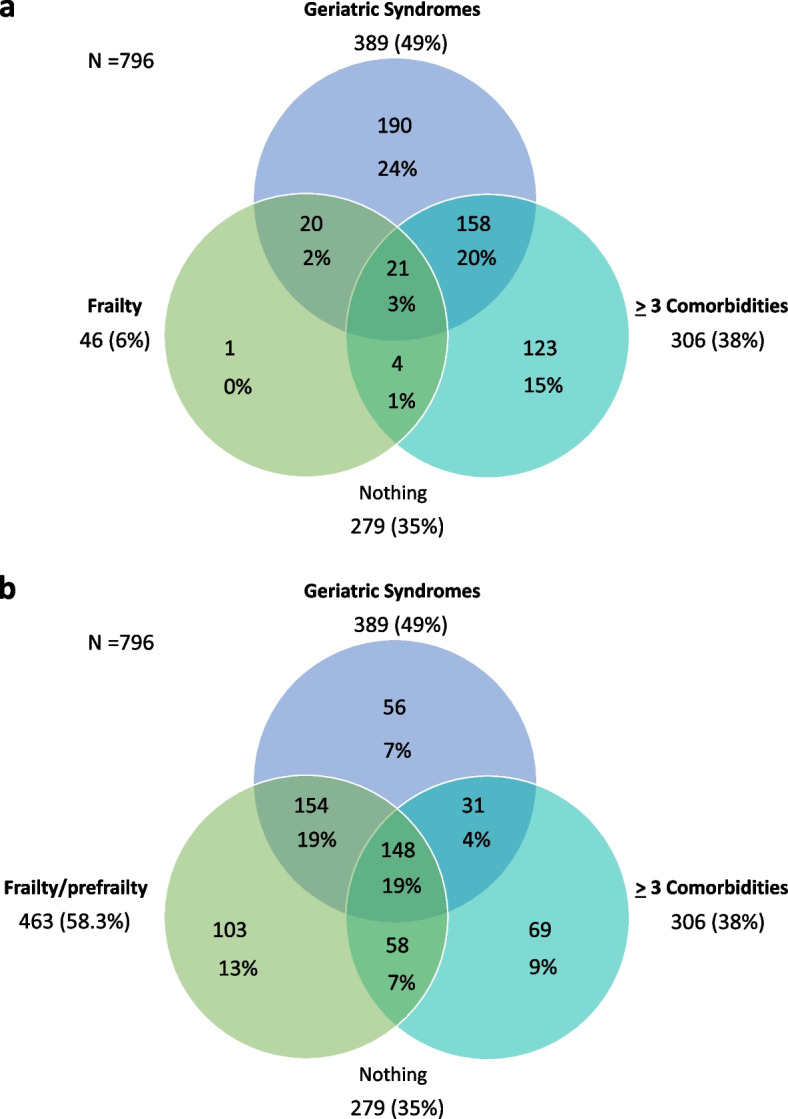
Methods: Cross-sectional study of the FUNCFRAIL multicenter cohort. The setting was outpatient HIV-Clinic. OAWH, 50 year or over were included. We recorded sociodemographic data, HIV infection-related data, comorbidity, frailty, geriatric syndromes (depression, cognitive impairment, falls and malnutrition), quality of life (QOL) and the estimated risk of all-cause 5-year mortality by VACS Index. Association of frailty with geriatric syndromes and comorbidity was evaluated using the Cochran-Mantel-Haenszel test.
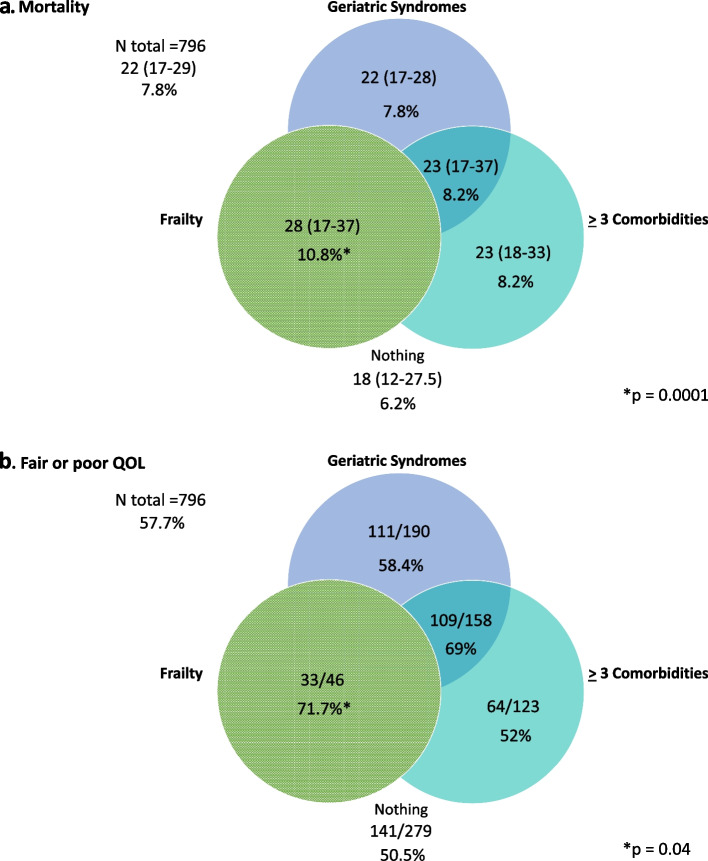
Results: Seven hundred ninety six patients were included. 24.7% were women, mean age was 58.2 (6.3). 14.7% were 65 or over. 517 (65%) patients had ≥3 comorbidities, ≥ 1 geriatric syndrome and/or frailty. There were significant differences in the estimated risk of mortality [(frailty 10.8%) vs. (≥ 3 comorbidities 8.2%) vs. (≥ 1 geriatric syndrome 8.2%) vs. (nothing 6.2%); p = 0.01] and in the prevalence of fair or poor QOL [(frailty 71.7%) vs. (≥ 3 comorbidities 52%) vs. (≥ 1 geriatric syndrome 58.4%) vs. (nothing 51%); p = 0.01]. Cognitive impairment was significantly associated to mortality (8.7% vs. 6.2%; p = 0.02) and depression to poor QOL [76.5% vs. 50%; p = 0.01].
Conclusions: Frailty, geriatric syndromes, and comorbidity had negative effects on mortality and QOL, but frailty had the greatest negative effect out of the three factors. Our results should be a wake-up call to standardize the screening for frailty and geriatric syndromes in OAWH in the clinical practice.
Trial registration: NCT03558438.
Keywords: Frailty; Geriatric syndromes; HIV; Mortality; Quality of life.
© 2023. The Author(s).
Conflict of interest statement
“The authors declare that they have no competing interests regarding this work”.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
