

Clustering of critically ill patients using an individualized learning approach enables dose optimization of mobilization in the ICU
- PMID: 36597110
- PMCID: PMC9808956
- DOI: 10.1186/s13054-022-04291-8
Clustering of critically ill patients using an individualized learning approach enables dose optimization of mobilization in the ICU
Abstract
Background: While early mobilization is commonly implemented in intensive care unit treatment guidelines to improve functional outcome, the characterization of the optimal individual dosage (frequency, level or duration) remains unclear. The aim of this study was to demonstrate that artificial intelligence-based clustering of a large ICU cohort can provide individualized mobilization recommendations that have a positive impact on the likelihood of being discharged home.
Methods: This study is an analysis of a prospective observational database of two interdisciplinary intensive care units in Munich, Germany. Dosage of mobilization is determined by sessions per day, mean duration, early mobilization as well as average and maximum level achieved. A k-means cluster analysis was conducted including collected parameters at ICU admission to generate clinically definable clusters.
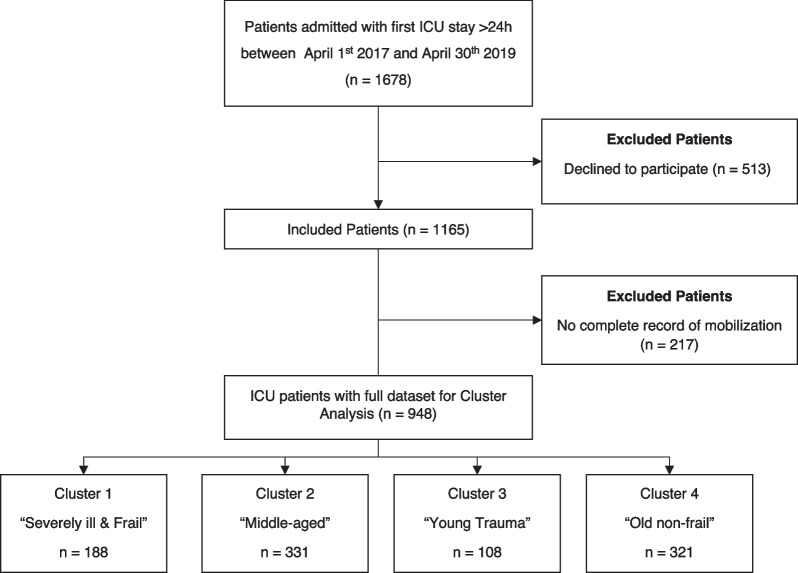
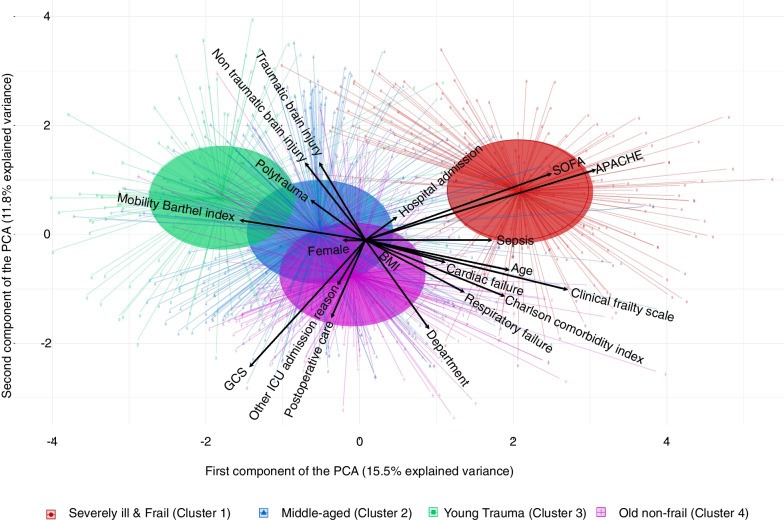
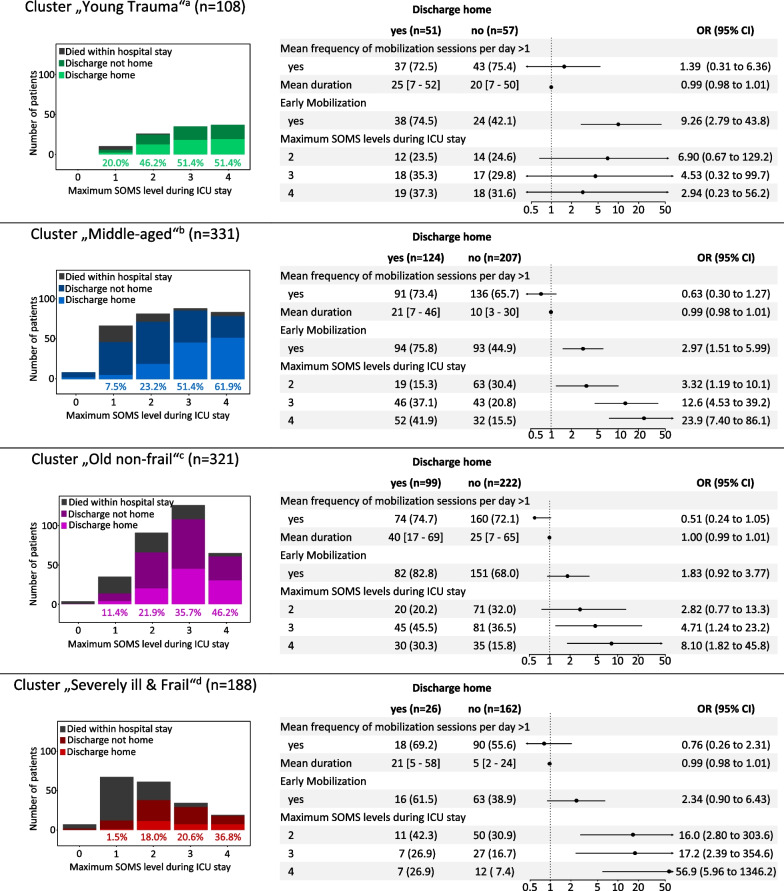
Results: Between April 2017 and May 2019, 948 patients were included. Four different clusters were identified, comprising "Young Trauma," "Severely ill & Frail," "Old non-frail" and "Middle-aged" patients. Early mobilization (< 72 h) was the most important factor to be discharged home in "Young Trauma" patients (ORadj 10.0 [2.8 to 44.0], p < 0.001). In the cluster of "Middle-aged" patients, the likelihood to be discharged home increased with each mobilization level, to a maximum 24-fold increased likelihood for ambulating (ORadj 24.0 [7.4 to 86.1], p < 0.001). The likelihood increased significantly when standing or ambulating was achieved in the older, non-frail cluster (ORadj 4.7 [1.2 to 23.2], p = 0.035 and ORadj 8.1 [1.8 to 45.8], p = 0.010).
Conclusions: An artificial intelligence-based learning approach was able to divide a heterogeneous critical care cohort into four clusters, which differed significantly in their clinical characteristics and in their mobilization parameters. Depending on the cluster, different mobilization strategies supported the likelihood of being discharged home enabling an individualized and resource-optimized mobilization approach.
Trial registration: Clinical Trials NCT03666286, retrospectively registered 04 September 2018.
Keywords: Critical care; Critical illness; Early ambulation; Patient discharge; Physical therapy modalities.
© 2023. The Author(s).
Conflict of interest statement
MB received research support from MSD (Haar, Germany) not related to this manuscript, received honoraria for giving lectures from GE Healthcare (Helsinki, Finland) and Grünenthal (Aachen, Germany). SJS received grants and non-financial support from Reactive Robotics GmbH (Munich, Germany), ASP GmbH (Attendorn, Germany), STIMIT AG (Biel, Switzerland), ESICM (Geneva, Switzerland), grants, personal fees and non-financial support from Fresenius Kabi Deutschland GmbH (Bad Homburg, Germany), personal fees from Springer Verlag GmbH (Vienna, Austria) for educational purposes and Advanz Pharma GmbH (Bielefeld, Germany), non-financial support from national and international societies (and their congress organizers) in the field of anesthesiology and intensive care medicine, outside the submitted work. Dr. Schaller held stocks in small amounts from Rhön-Klinikum AG and holds stocks in small amounts from Alphabeth Inc., Bayer AG and Siemens AG; these holdings have not affected any decisions regarding his research or this study. The other authors declare that they have no competing interests.
Figures
References
-
- Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874–1882. doi: 10.1016/S0140-6736(09)60658-9. - DOI - PMC - PubMed
-
- Schaller SJ, Anstey M, Blobner M, Edrich T, Grabitz SD, Gradwohl-Matis I, Heim M, Houle T, Kurth T, Latronico N, et al. Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016;388(10052):1377–1388. doi: 10.1016/S0140-6736(16)31637-3. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
