

Incomplete Antiretroviral Therapy Adherence Is Associated with Lower CD4-CD8 Ratio in Virally Suppressed Patients with HIV Infection in Mexico
- PMID: 36597354
- PMCID: PMC9986006
- DOI: 10.1089/AID.2021.0179
Incomplete Antiretroviral Therapy Adherence Is Associated with Lower CD4-CD8 Ratio in Virally Suppressed Patients with HIV Infection in Mexico
Abstract
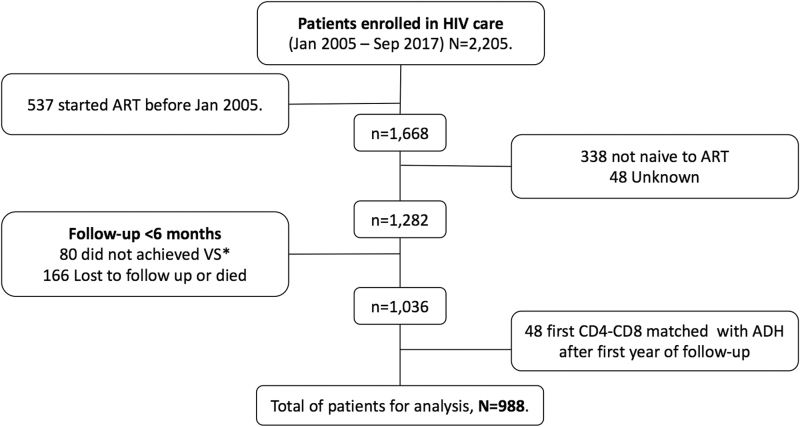
Suboptimal adherence to antiretroviral therapy (ART) in people with HIV, even during sustained viral suppression, is associated with persistent inflammation, immune activation, and coagulopathy. Persistently low CD4-CD8 Ratio has been also associated with residual inflammation, is a good predictor of increased risk of death and more widely available than inflammatory biomarkers. We tested the hypothesis that the CD4-CD8 Ratio is associated with ART adherence during periods of complete viral suppression. We used the Medication Possession Ratio based in pharmacy registries as measure of adherence and time-varying, routine care CD4 and CD8 measurements as outcome. We used a linear mixed model for longitudinal data, including fixed effects for sex, age, education, date of ART initiation, AIDS-related conditions, and baseline CD4 to model the outcome. In 988 adults with a median follow-up of 4.13 years, higher ART adherence was independently associated with a modest increase in CD4-CD8. For each increasing percentage point in adherence, the CD4-CD8 Ratio increased 0.000857 (95% confidence interval [CI] -0.000494 to 0.002209, p = .213731) in the first year after achieving viral suppression; 0.001057 (95% CI 0.000262-0.001853, p = .009160) in years 1 to 3; 0.000323 (95% CI -0.000448 to 0.001095, p = .411441) in years 3 to 5; and 0.000850 (95% CI 0.000272-0.001429, p = .003946) 5-10 years after achieving viral suppression. The magnitude of the effect of adherence over CD4-CD8 Ratios varied over time and by baseline CD4 count, with increasing adherence having a larger effect early after ART initiation in people with higher baseline CD4 (>500 cells/μL) and in later years in people with lower baseline CD4 count (≥200 cells/μL). Our findings expand on previous evidence suggesting that the benefits of optimal adherence to modern ART regimens goes beyond maintaining viral suppression. These results highlight the importance of including objective measurements of adherence as part of routine care, even in patients with complete HIV suppression over long-term follow-up.
Keywords: acquired immunodeficiency syndrome; adult; cohort studies; linear mixed models; pharmacy; sustained virologic response.
Conflict of interest statement
No competing financial interests exist.
Figures



References
-
- Younas M, Psomas C, Reynes J, et al. . Immune activation in the course of HIV-1 infection: Causes, phenotypes and persistence under therapy. HIV Med 2016;17(2): 89–105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
