

Interactive Effects of Molecular, Therapeutic, and Patient Factors on Outcome of Diffuse Low-Grade Glioma
- PMID: 36599113
- PMCID: PMC10082290
- DOI: 10.1200/JCO.21.02929
Interactive Effects of Molecular, Therapeutic, and Patient Factors on Outcome of Diffuse Low-Grade Glioma
Abstract
Purpose: In patients with diffuse low-grade glioma (LGG), the extent of surgical tumor resection (EOR) has a controversial role, in part because a randomized clinical trial with different levels of EOR is not feasible.
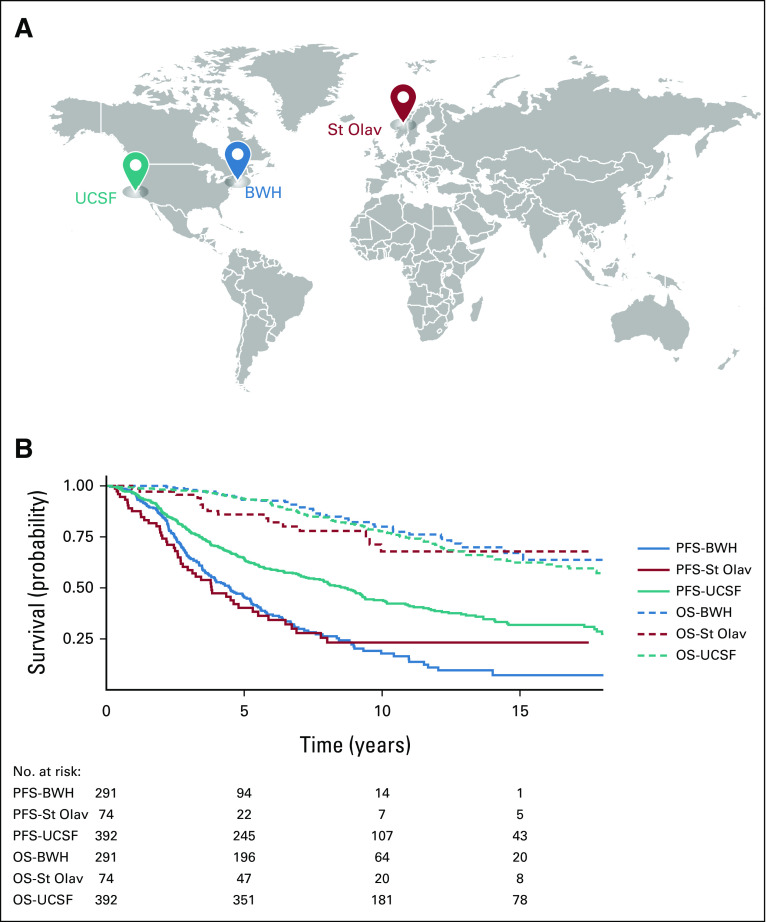
Methods: In a 20-year retrospective cohort of 392 patients with IDH-mutant grade 2 glioma, we analyzed the combined effects of volumetric EOR and molecular and clinical factors on overall survival (OS) and progression-free survival by recursive partitioning analysis. The OS results were validated in two external cohorts (n = 365). Propensity score analysis of the combined cohorts (n = 757) was used to mimic a randomized clinical trial with varying levels of EOR.
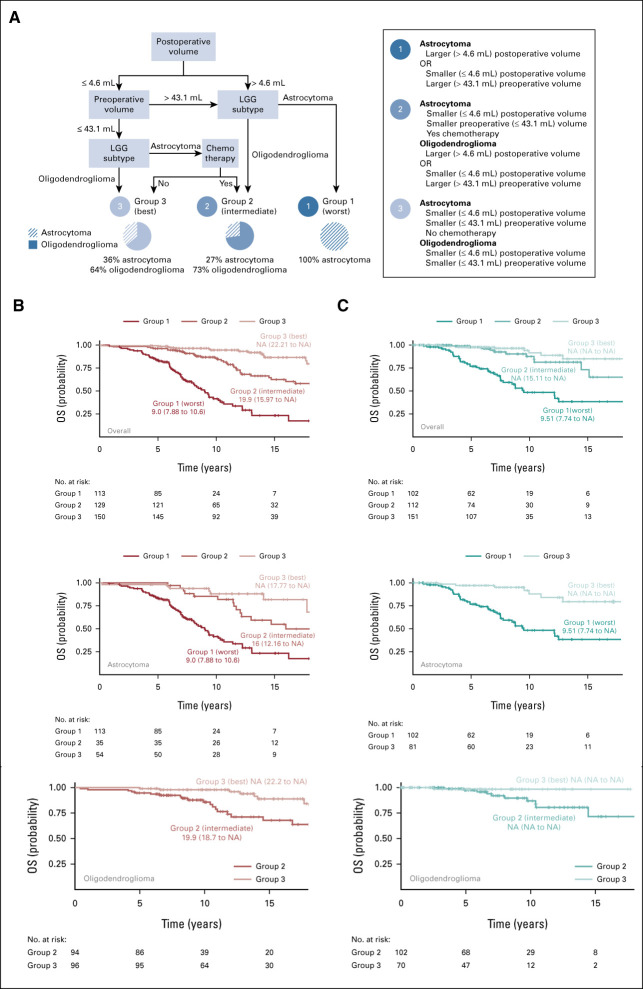
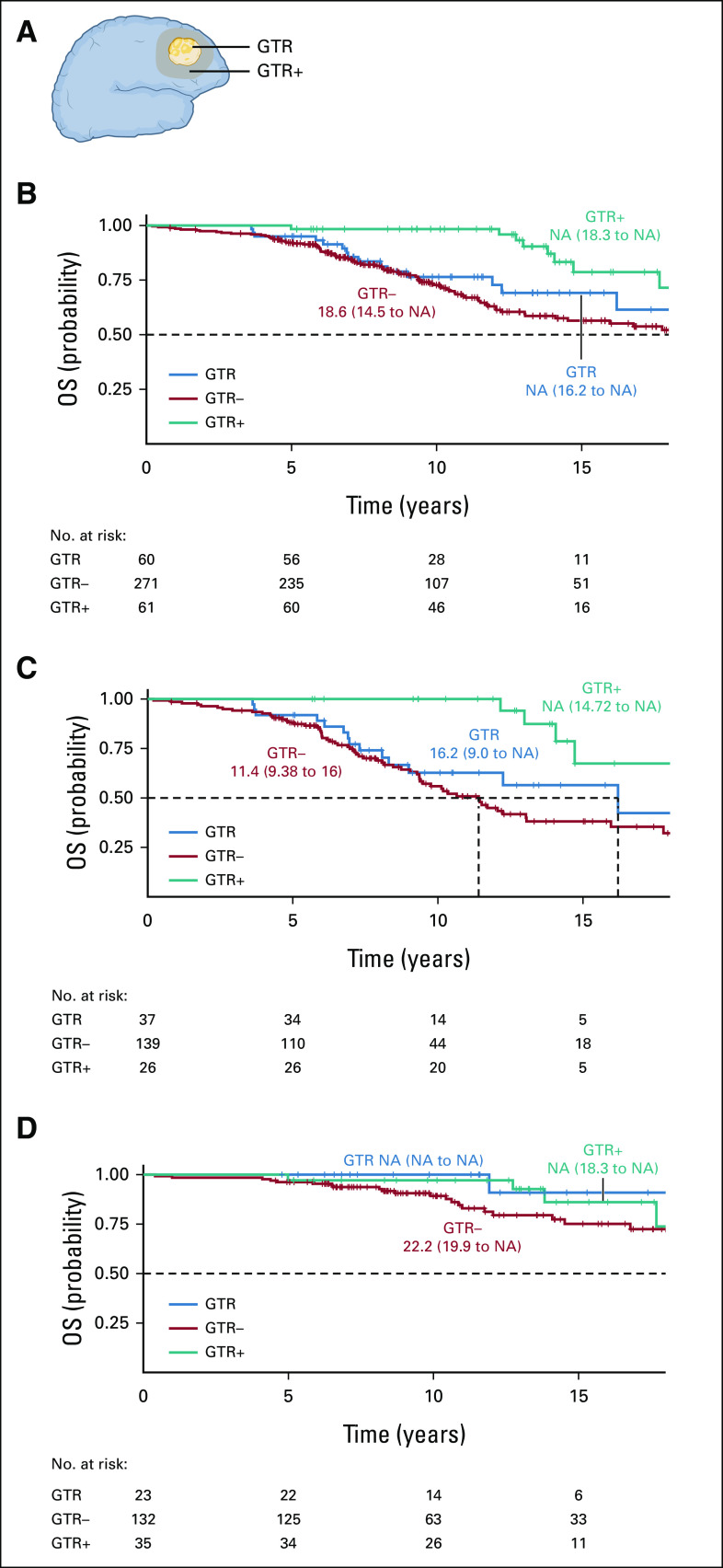
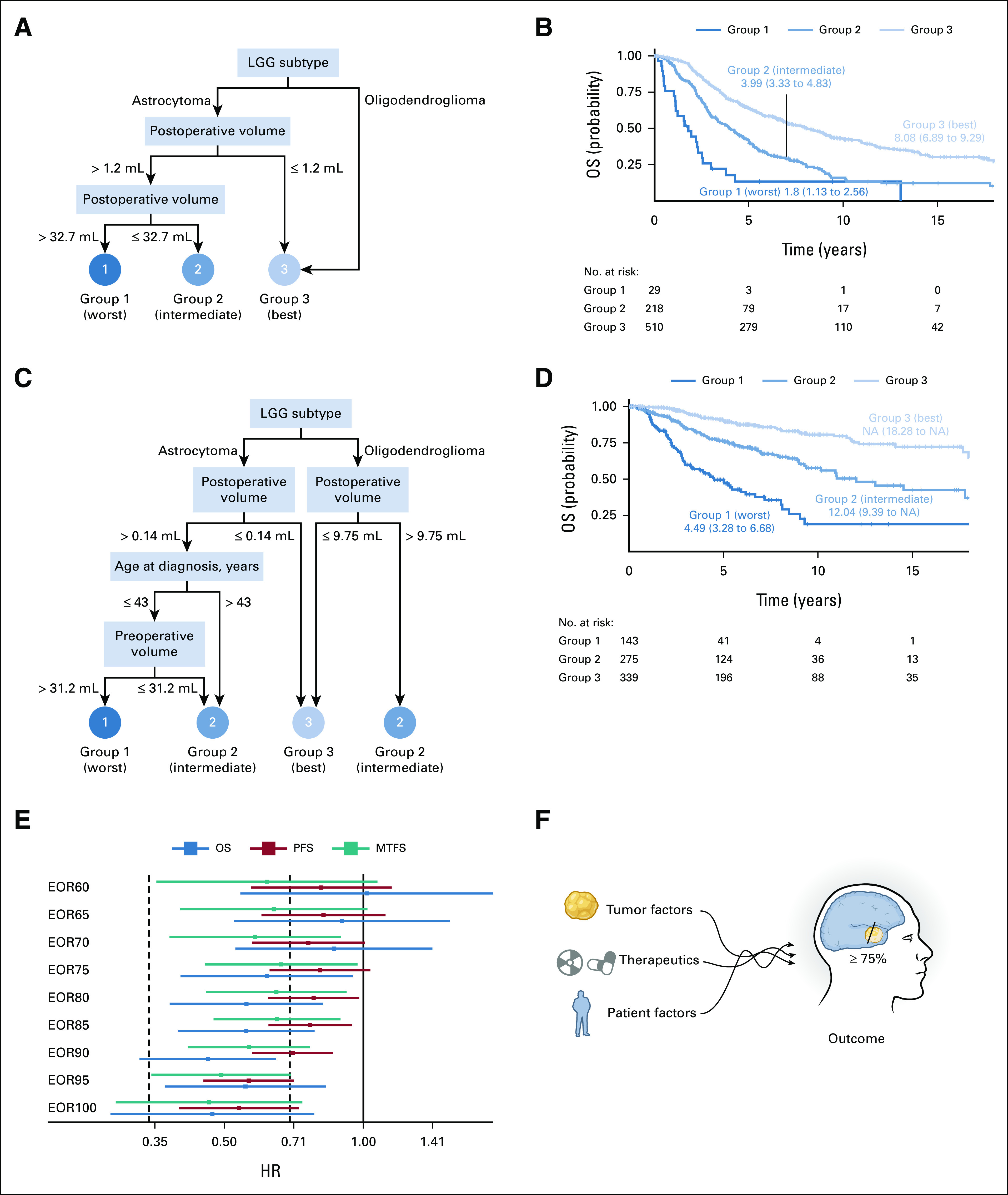
Results: Recursive partitioning analysis identified three survival risk groups. Median OS was shortest in two subsets of patients with astrocytoma: those with postoperative tumor volume (TV) > 4.6 mL and those with preoperative TV > 43.1 mL and postoperative TV ≤ 4.6 mL. Intermediate OS was seen in patients with astrocytoma who had chemotherapy with preoperative TV ≤ 43.1 mL and postoperative TV ≤ 4.6 mL in addition to oligodendroglioma patients with either preoperative TV > 43.1 mL and residual TV ≤ 4.6 mL or postoperative residual volume > 4.6 mL. Longest OS was seen in astrocytoma patients with preoperative TV ≤ 43.1 mL and postoperative TV ≤ 4.6 mL who received no chemotherapy and oligodendroglioma patients with preoperative TV ≤ 43.1 mL and postoperative TV ≤ 4.6 mL. EOR ≥ 75% improved survival outcomes, as shown by propensity score analysis.
Conclusion: Across both subtypes of LGG, EOR beginning at 75% improves OS while beginning at 80% improves progression-free survival. Nonetheless, maximal resection with preservation of neurological function remains the treatment goal. Our findings have implications for surgical strategies for LGGs, particularly oligodendroglioma.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
Comment in
-
Long-Term Outcomes in Resected IDH-Mutant Subtypes of Diffuse Low-Grade Glioma.J Clin Oncol. 2023 Apr 10;41(11):1979-1981. doi: 10.1200/JCO.22.02428. Epub 2023 Feb 28. J Clin Oncol. 2023. PMID: 36854064 No abstract available.
References
-
- Louis DN, Wiestler OD, Cavenee WK: World Health Organization Histological Classification of Tumours of the Central Nervous System (ed 4 revised). Lyon, France, International Agency for Research on Cancer, 2016
Publication types
MeSH terms
Grants and funding
- HHSN261201800032C/CA/NCI NIH HHS/United States
- HHSN261201800009C/CA/NCI NIH HHS/United States
- NU58DP006344/DP/NCCDPHP CDC HHS/United States
- T32 CA151022/CA/NCI NIH HHS/United States
- R25 CA112355/CA/NCI NIH HHS/United States
- HHSN261201800015I/CA/NCI NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- P50 CA097257/CA/NCI NIH HHS/United States
- R01 CA207360/CA/NCI NIH HHS/United States
- HHSN261201800032I/CA/NCI NIH HHS/United States
- L30 CA199570/CA/NCI NIH HHS/United States
- HHSN261201800015C/CA/NCI NIH HHS/United States
- HHSN261201800009I/CA/NCI NIH HHS/United States
- K08 NS110919/NS/NINDS NIH HHS/United States
