

Safety, Efficacy, and Tolerability of Modified Atkins Diet in Persons With Drug-Resistant Epilepsy: A Randomized Controlled Trial
- PMID: 36599697
- PMCID: PMC10065201
- DOI: 10.1212/WNL.0000000000206776
Safety, Efficacy, and Tolerability of Modified Atkins Diet in Persons With Drug-Resistant Epilepsy: A Randomized Controlled Trial
Abstract
Background and objectives: Modified Atkins diet (MAD) has emerged as an adjuvant therapy in drug-resistant epilepsy (DRE). Most studies are in children; there is limited evidence for DRE in adults. This study aimed to investigate whether MAD along with standard drug therapy (SDT) was indeed more effective than SDT alone in reducing seizure frequency and improving psychological outcomes at 6 months in adolescents and adults with DRE (nonsurgical).
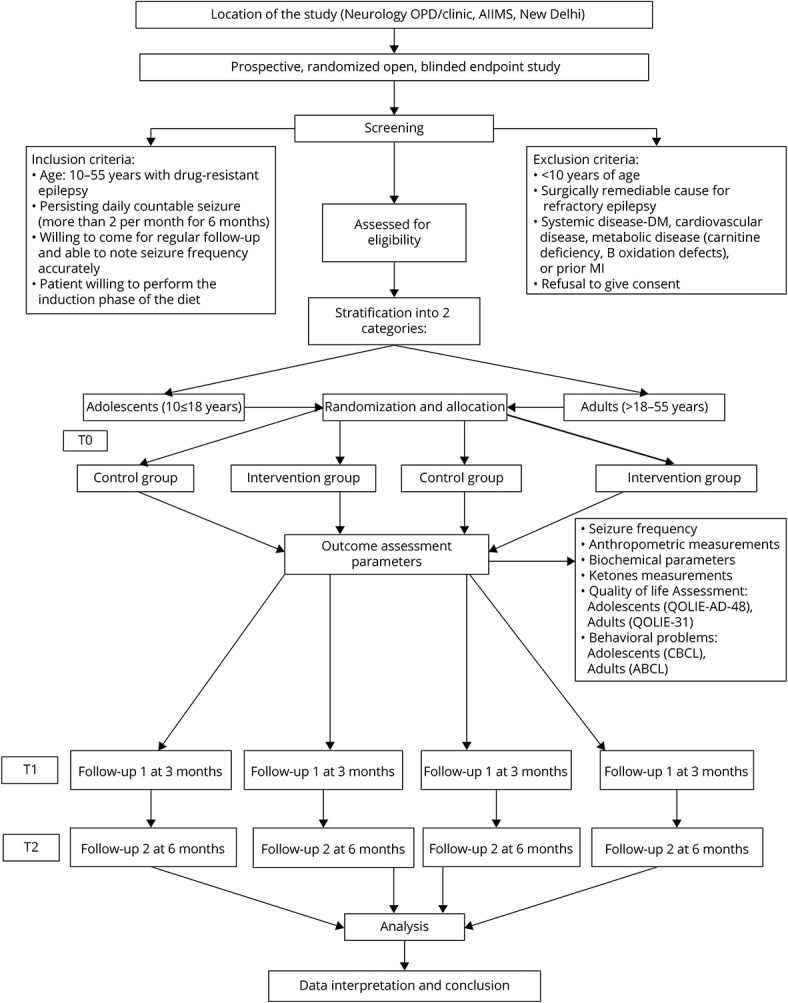
Methods: A prospective randomized controlled trial was conducted at tertiary care referral center in India. Persons with DRE aged 10-55 years attending outpatient epilepsy clinics between August 2015 and April 2019, who had more than 2 seizures per month despite using at least 3 appropriate antiseizure medications (ASMs) at their maximum tolerated doses and had not been on any form of diet therapy for the past 1 year, were enrolled. Patients were assessed for the eligibility and randomly assigned to receive SDT plus MAD (intervention arm) or SDT alone (control arm). The primary outcome was >50% reduction in seizure frequency, and the secondary outcomes were quality of life (QOL), behavior, adverse events, and rate of withdrawal at 6 months. Intention-to-treat analysis was performed.
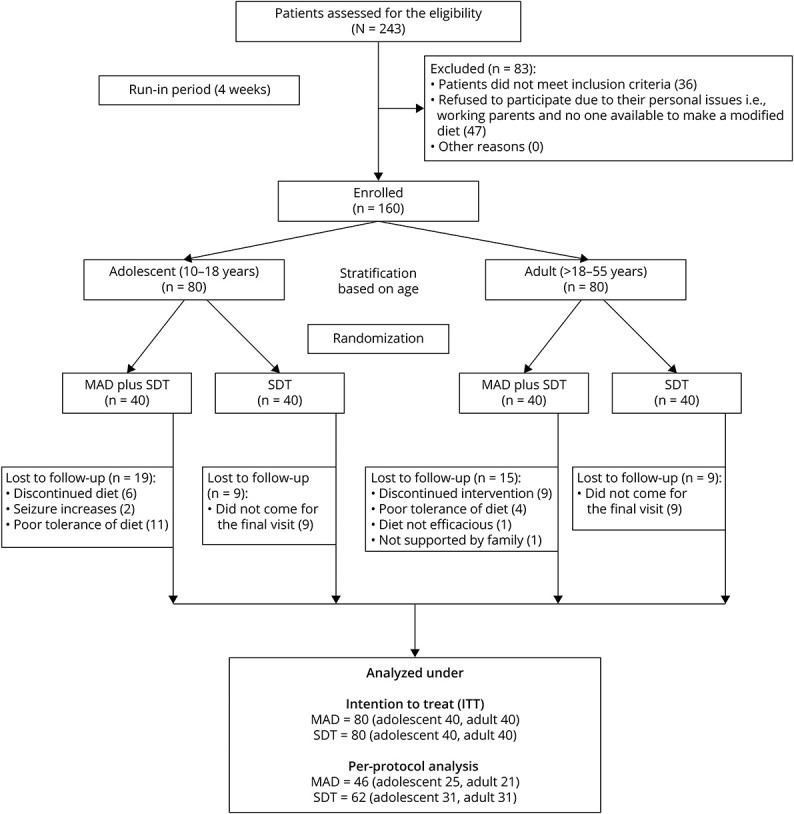
Results: A total of 243 patients were screened for eligibility; 160 patients (80 adults and 80 adolescents) were randomized to either the intervention or control arm. Demographic and clinical characteristics in both groups were comparable at baseline. At 6 months, >50% seizure reduction was seen in 26.2% in the intervention group vs 2.5% in the control group (95% CI 13.5-33.9; p < 0.001). Improvement in QOL was 52.1 ± 17.6 in the intervention group vs 42.5 ± 16.4 in the control group (mean difference, 9.6; 95% CI 4.3 to 14.9, p < 0.001). However, behavior scores could be performed in 49 patients, and improvement was seen in the intervention vs control group (65.6 ± 7.9 vs 71.4 ± 8.1, p = 0.015) at the end of the study. One patient had weight loss; 2 patients had diarrhea.
Discussion: The MAD group demonstrated improvement in all aspects (reduction in seizure frequency and behavioral problems) compared with the control group at the end of the study. MAD is an effective modality in controlling seizures; further research is required to assess its efficacy in terms of biomarkers along with descriptive metabolomics studies.
Trial registration information: The clinical trial registry of India: CTRI/2015/07/006048.
Classification of evidence: This study provides Class III evidence that the MAD increases the probability of seizure reduction in adolescents and adults with DRE.
© 2023 American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures
Comment in
-
Keto Is Not Just for Kids: A Randomized Trial of a Modified Atkins Diet for Adolescents and Adults With Anti-Seizure Medication-Resistant Epilepsy.Epilepsy Curr. 2023 Mar 5;23(3):147-149. doi: 10.1177/15357597231157488. eCollection 2023 May-Jun. Epilepsy Curr. 2023. PMID: 37334414 Free PMC article. No abstract available.
References
-
- Kossoff EH, Zupec‐Kania BA, Auvin S, et al. ; The Charlie Foundation Matthew's Friends the Practice Committee of the Child Neurology Society. Optimal clinical management of children receiving dietary therapies for epilepsy: updated recommendations of the International Ketogenic Diet Study Group. Epilepsia Open. 2018;3(2):175-192. doi: 10.1002/epi4.12225 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous