

Variability of radiotherapy volume delineation: PSMA PET/MRI and MRI based clinical target volume and lymph node target volume for high-risk prostate cancer
- PMID: 36600283
- PMCID: PMC9811734
- DOI: 10.1186/s40644-022-00518-7
Variability of radiotherapy volume delineation: PSMA PET/MRI and MRI based clinical target volume and lymph node target volume for high-risk prostate cancer
Abstract
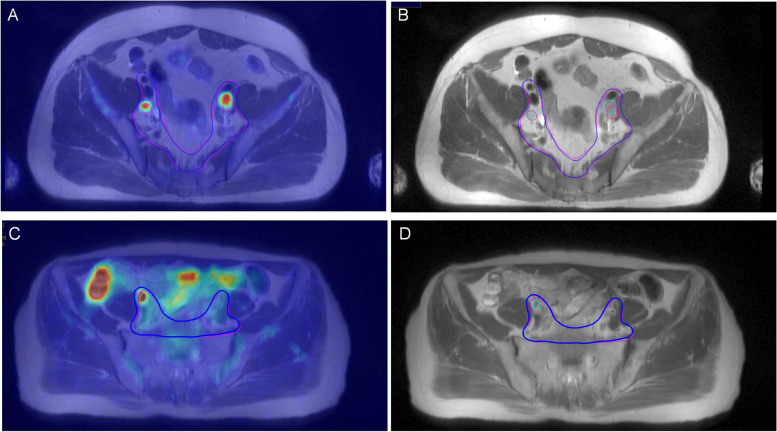
Purpose: A comparative retrospective study to assess the impact of PSMA Ligand PET/MRI ([68 Ga]-Ga-PSMA-11 and [18F]-F-PSMA-1007 PET/MRI) as a new method of target delineation compared to conventional imaging on whole-pelvis radiotherapy for high-risk prostate cancer (PCa).
Patients and methods: Forty-nine patients with primary high-risk PCa completed the whole-pelvis radiotherapy plan based on PSMA PET/MRI and MRI. The primary endpoint compared the size and overlap of clinical target volume (CTV) and nodal gross tumour volume (GTVn) based on PSMA PET/MRI and MRI. The diagnostic performance of two methods for pelvic lymph node metastasis (PLNM) was evaluated.
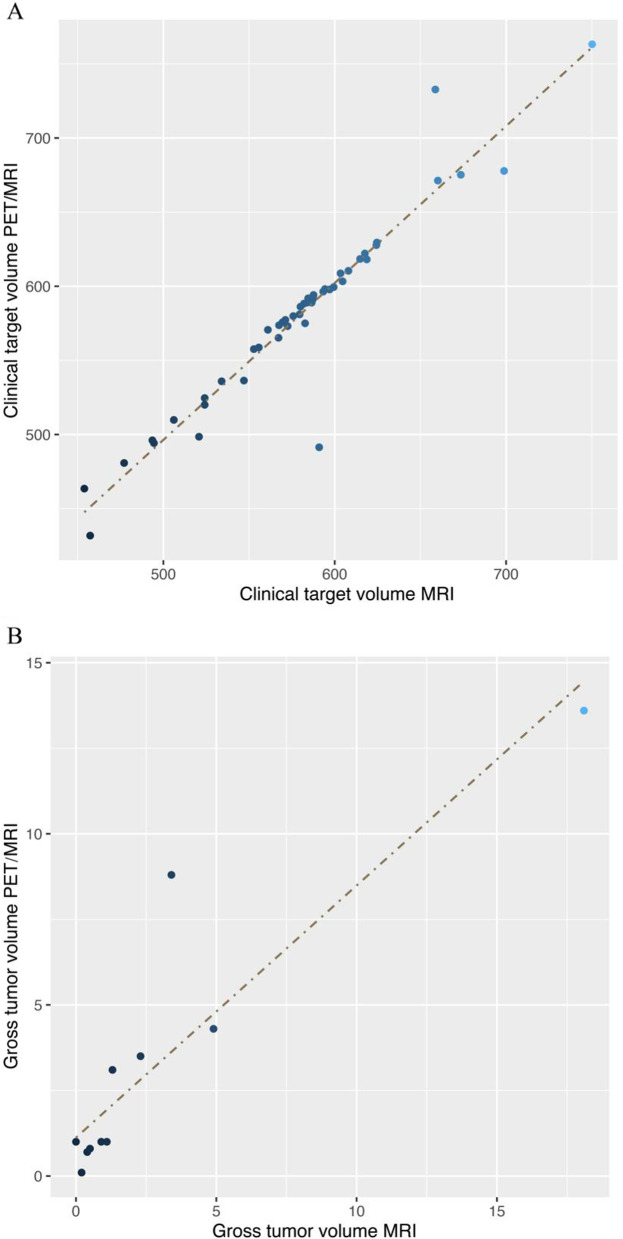
Results: In the radiotherapy planning for high-risk PCa patients, there was a significant correlation between MRI-CTV and PET/MRI-CTV (P = 0.005), as well as between MRI-GTVn and PET/MRI-GTVn (P < 0.001). There are non-significant differences in the CTV and GTVn based on MRI and PET/MRI images (P = 0.660, P = 0.650, respectively). The conformity index (CI), lesion coverage factor (LCF) and Dice similarity coefficient (DSC) of CTVs were 0.999, 0.953 and 0.954. The CI, LCF and DSC of GTVns were 0.927, 0.284, and 0.32. Based on pathological lymph node analysis of 463 lymph nodes from 37 patients, the sensitivity, specificity of PET/MRI in the diagnosis of PLNM were 77.78% and 99.76%, respectively, which were higher than those of MRI (P = 0.011). Eight high-risk PCa patients who finished PSMA PET/MRI changed their N or M stage.
Conclusion: The CTV delineated based on PET/MRI and MRI differ little. The GTVn delineated based on PET/MRI encompasses metastatic pelvic lymph nodes more accurately than MRI and avoids covering pelvic lymph nodes without metastasis. We emphasize the utility of PET/MRI fusion images in GTVn delineation in whole pelvic radiotherapy for PCa. The use of PSMA PET/MRI aids in the realization of more individual and precise radiotherapy for PCa.
Keywords: CTV; GTVn; PET/MRI; PSMA; Prostate cancer; Radiotherapy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Figures




References
-
- Chughtai B, Mian BM. High risk prostate cancer: evolving definition and approach to management. Can J Urol. 2008;15(6):4375–4380. - PubMed
-
- Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, et al. EAU guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol. 2014;65(1):124–37. 10.1016/j.eururo.2013.09.046. Epub 2013 Oct 6. - PubMed
MeSH terms
Substances
Grants and funding
- 81960525/National Natural Science Foundation of China
- 82160591/National Natural Science Foundation of China
- 19DZ1930900/Science and Technology Commission of Shanghai Municipality
- DFLC2022012/Shanghai Key Laboratory of Gynecologic Oncology
- PWZzk2022-02/Health and Family Planning Committee of Pudong New Area
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
