

Efficacy and safety of lifileucel, a one-time autologous tumor-infiltrating lymphocyte (TIL) cell therapy, in patients with advanced melanoma after progression on immune checkpoint inhibitors and targeted therapies: pooled analysis of consecutive cohorts of the C-144-01 study
- PMID: 36600653
- PMCID: PMC9748991
- DOI: 10.1136/jitc-2022-005755
Efficacy and safety of lifileucel, a one-time autologous tumor-infiltrating lymphocyte (TIL) cell therapy, in patients with advanced melanoma after progression on immune checkpoint inhibitors and targeted therapies: pooled analysis of consecutive cohorts of the C-144-01 study
Abstract
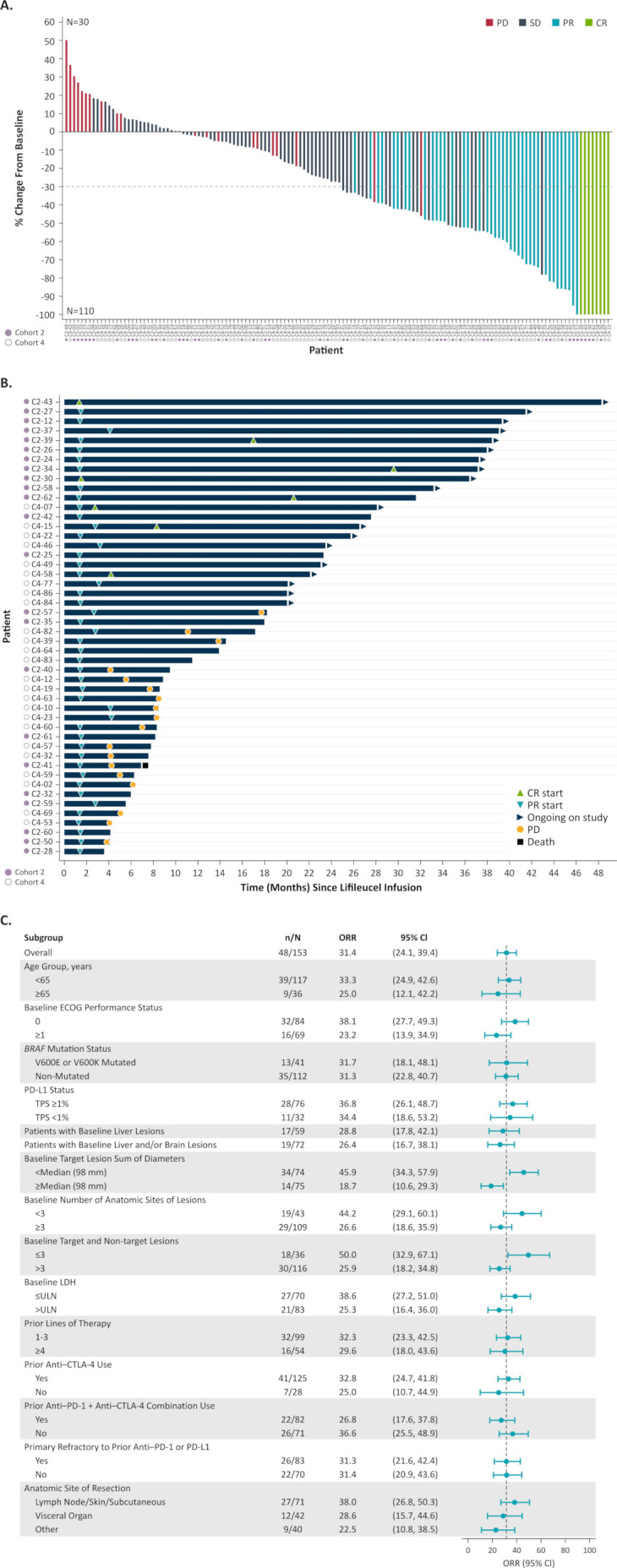
Background: Patients with advanced melanoma have limited treatment options after progression on immune checkpoint inhibitors (ICI). Lifileucel, a one-time autologous tumor-infiltrating lymphocyte (TIL) cell therapy, demonstrated an investigator-assessed objective response rate (ORR) of 36% in 66 patients who progressed after ICI and targeted therapy. Herein, we report independent review committee (IRC)-assessed outcomes of 153 patients treated with lifileucel in a large multicenter Phase 2 cell therapy trial in melanoma.
Methods: Eligible patients had advanced melanoma that progressed after ICI and targeted therapy, where appropriate. Melanoma lesions were resected (resected tumor diameter ≥1.5 cm) and shipped to a central good manufacturing practice facility for 22-day lifileucel manufacturing. Patients received a non-myeloablative lymphodepletion regimen, a single lifileucel infusion, and up to six doses of high-dose interleukin-2. The primary endpoint was IRC-assessed ORR (Response Evaluation Criteria in Solid Tumors V.1.1).
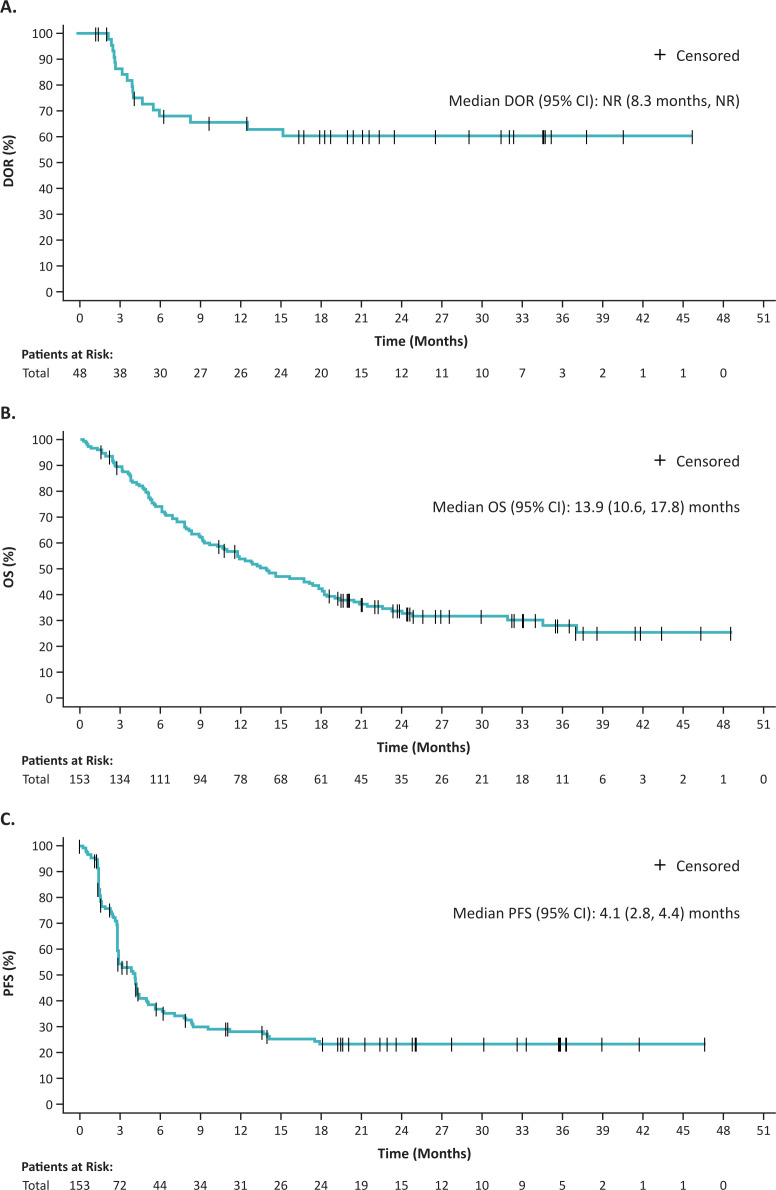
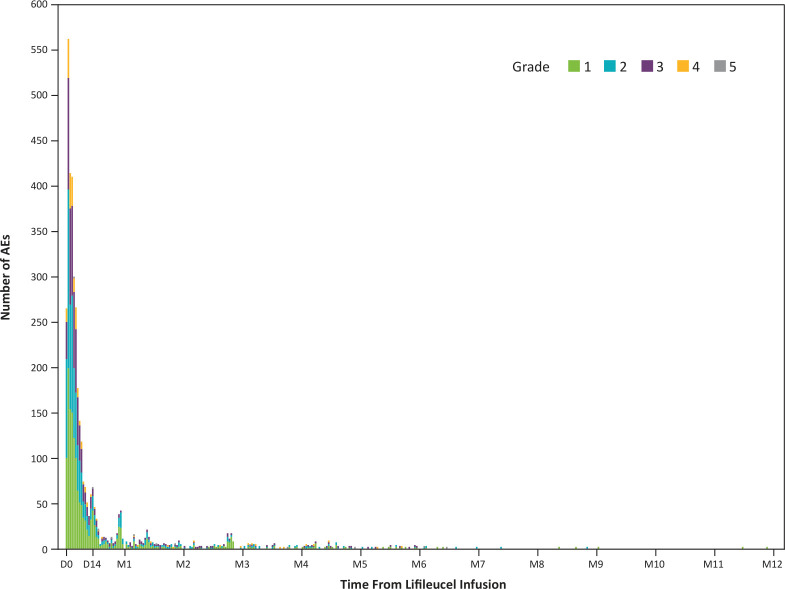
Results: The Full Analysis Set consisted of 153 patients treated with lifileucel, including longer-term follow-up on the 66 patients previously reported. Patients had received a median of 3.0 lines of prior therapy (81.7% received both anti-programmed cell death protein 1 and anti-cytotoxic lymphocyte-associated protein 4) and had high disease burden at baseline (median target lesion sum of diameters (SOD): 97.8 mm; lactate dehydrogenase (LDH) >upper limit of normal: 54.2%). ORR was 31.4% (95% CI: 24.1% to 39.4%), with 8 complete responses and 40 partial responses. Median duration of response was not reached at a median study follow-up of 27.6 months, with 41.7% of the responses maintained for ≥18 months. Median overall survival and progression-free survival were 13.9 and 4.1 months, respectively. Multivariable analyses adjusted for Eastern Cooperative Oncology Group performance status demonstrated that elevated LDH and target lesion SOD >median were independently correlated with ORR (p=0.008); patients with normal LDH and SOD <median had greater likelihood of response than those with either (OR=2.08) or both (OR=4.42) risk factors. The most common grade 3/4 treatment-emergent adverse events (≥30%) were thrombocytopenia (76.9%), anemia (50.0%), and febrile neutropenia (41.7%).
Conclusions: Investigational lifileucel demonstrated clinically meaningful activity in heavily pretreated patients with advanced melanoma and high tumor burden. Durable responses and a favorable safety profile support the potential benefit of one-time lifileucel TIL cell therapy in patients with limited treatment options in ICI-refractory disease.
Keywords: Clinical Trials, Phase II as Topic; Immunotherapy; Immunotherapy, Adoptive; Lymphocytes, Tumor-Infiltrating; Melanoma.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JC reports consulting or advisory role with Amgen and research funding from Replimune, Amgen, Iovance Biotherapeutics, and Fate Therapeutics. KDL reports receiving honoraria from Array BioPharma and Iovance Biotherapeutics; consulting or advisory role with Array BioPharma, Merck, Roche, Regeneron, Sanofi, Iovance Biotherapeutics, and Nektar; research funding from Roche/Genentech, Merck, Array BioPharma, Incyte, Nektar, Iovance Biotherapeutics, Bristol-Myers Squibb, Kartos Therapeutics, OncoSec, Regeneron, Alkermes, Neon Therapeutics, Ultimovacs, Senhwa Biosciences, Replimune, Amgen, and Seagen; travel, accommodations, and expenses from Merck, Roche/Genentech, Regeneron, Neon Therapeutics, and Alkermes; and uncompensated relationships with Roche/Genentech and Regeneron. HK reports consulting or advisory role with Bristol-Myers Squibb, Clinigen, Shionogi, Chemocentryx, Calithera, Signatera, GigaGen, GI Reviewers, and Merck; and research funding from Apexigen, Bristol-Myers Squibb, and Merck. OH reports receiving honoraria and has consulting or advisory role with Aduro, Akeso, Alkermes, Amgen, BeiGene, BioAtla, Bristol-Myers Squibb, Roche Genentech, GlaxoSmithKline, Immunocore, Idera, Incyte, InstilBio, Iovance Biotherapeutics, Janssen, Merck, Nextcure, Novartis, Pfizer, Sanofi/Regeneron, Seagen, Tempus, and Zelluna; research funding from Arcus, Aduro, Akeso, Amgen, Bioatla, Bristol-Myers Squibb, CytomX, Exelixis, Roche Genentech, GSK, Immunocore, Idera, Incyte, Iovance Biotherapeutics, Merck, Moderna, Merck-Serono, NextCure, Novartis, Pfizer, Rubius, Sanofi-Regeneron, and Seagen; and is on the speaker’s bureau for Bristol-Myers Squibb, Novartis, Pfizer, and Sanofi Regeneron. EW reports consultant or advisory role with Merck; research funding received as site principal investigator for multiple studies (>30); and being on the speaker’s bureau for Bristol-Myers Squibb, Regeneron, and Castle Biosciences. ST reports honoraria, consulting or advisory role, research funding, speaker’s bureau, and travel, accommodations, expenses with Bristol-Myers Squibb, Merck, Pfizer, Ipsen, Amgen, Genentech, and Foundation One. MW reports receiving honoraria from Novartis, Pfizer, and Roche; consulting or advisory role with Bristol-Myers Squibb, Novartis, Pfizer, Cellex GmbH, Eli Lilly, Boehringer Ingelheim, ISA Pharmaceuticals, GEMoaB, Roche, MSD, AstraZeneca, Amgen, and Immatics; research funding from Roche; and travel, accommodations, and expenses from Pfizer, Bristol-Myers Squibb, AstraZeneca, Roche, Amgen, and GEMoaB. MC reports speaker’s bureau participation with Sirtex Medical. ED-M reports receiving honoraria from Castle Biosciences; consulting or advisory role and speaker’s bureau with Regeneron; and research funding from Clinigen. GQP reports honoraria from IBSA; consulting or advisory role with Acella, Amneal, and Terns; and patents, royalties, or other intellectual property with Virginia Commonwealth University. JMK reports consulting role with Amgen, Ankyra Therapeutics, Applied Clinical Intelligence, Axio Research, Becker Pharmaceutical Consulting, Bristol-Myers Squibb, Cancer Network, Checkmate Pharmaceuticals, DermTech, Fenix Group International, Harbour BioMed, Immunocore, Iovance Biotherapeutics, IQVIA, Istari Oncology, Merck, Natera, Novartis, Oncocyte, OncoSec, Pfizer, Replimune, Scopus BioPharma, SR One Capital Management LP, Takeda Development Center Americas, and Takeda Pharmaceutical Company; and research trial support to institution from Amgen, Bristol-Myers Squibb, Checkmate Pharmaceuticals, Harbour BioMed, ImmVira, Immunocore, Iovance Biotherapeutics, Novartis, Takeda, and Verastem. JCH reports honorarias for talks from Almirall, Amgen, Bristol-Myers Squibb, GSK, JSD Pharma, Novartis, Pierre Fabre, Roche, Sanofi, and Sun Pharma; advisory boards for GSK, MSD, Pierre Fabre, Sun Pharma (personal), and Bristol-Myers Squibb, Immunocore, Nektar, Novartis, and Philogen (institution); research funding from Bristol-Myers Squibb, Sun Pharma, and Sanofi; and travel, accommodations, and expenses from Sun Pharma. MO reports consulting or advisory role with TriSalus, Immunocore, Ideaya, and Delcath, and her husband is an employee of GSK. JL reports receiving honoraria from Eisai, Novartis, Incyte, Merck, touchIME, touchEXPERTS, Royal College of Physicians, Cambridge Healthcare Research, Royal College of General Practitioners, VJOncology, Agence Unik, and Bristol-Myers Squibb; consulting or advisory role with iOnctura, Apple Tree, Merck, Bristol-Myers Squibb, Eisai, Debiopharm, and Incyte; research funding from Bristol-Myers Squibb, MSD, Novartis, Pfizer, Achilles Therapeutics, Roche, Nektar, Covance, Immunocore, Pharmacyclics, and Aveo; and travel, accommodations, and expenses from Pierre Fabre, Roche, and GSK. JW reports stock or other ownership with Biond, Instil Bio, OncoV4, and Evaxion; honoraria and consulting or advisory role with Bristol-Myers Squibb, GSK, Pfizer, Sellas, Biond, OncoC4, ImCheck, Genentech, AstraZeneca, Regeneron, Instil Bio, Iovance Biotherapeutics, Evaxion, and Ultimovacs; research funding from Bristol-Myers Squibb, Moderna, Merck, Incyte, and Genentech; patents, royalties, or other intellectual property with Moffitt Cancer Center and Biodesix. AJSF reports consulting or advisory role with Immunocore and GSK; speaker’s bureau participation with Bristol-Myers Squibb, Ipsen, and Eisai; and travel, accommodations, and expenses from ESMO. NIK reports stock and other ownership interest with Bellicum Pharmaceuticals, Amarin Corporation, and Asensus Surgical; consulting or advisory role with Bristol-Myers Squibb, AstraZeneca, Regeneron, Array BioPharma, Immunocore, Merck, Incyte, Jounce Therapeutics, Iovance Biotherapeutics, NCCN/Pfizer, Genzyme, Novartis, Nektar, Castle Biosciences, and InstilBio; research funding from Bristol-Myers Squibb, Merck, Novartis, GSK, HUYA Bioscience International, Amgen, Regeneron, Celgene, and Replimune; and other relationships with Nektar, Regeneron, Bristol-Myers Squibb/Celgene, and Replimune. TM reports consulting or advisory role with Merck, Bristol-Myers Squibb, Iovance Biotherapeutics, Moderna, Nektar, Regeneron, Exicure, Checkmate Pharmaceuticals, BioAtla, Xencor, Replimune, Day One Biopharmaceuticals, Pfizer, and Taiga. MEE reports consultant or advisory role with Iovance Biotherapeutics and receiving research funding from SkylineDx. FGF, MJ, PH, GS, WS, and XW are employees of Iovance Biotherapeutics and hold stock and/or stock options. Further, FGF is in a leadership position at Iovance Biotherapeutics; owns stocks from Adverum Biotechnologies, Roche, Bristol-Myers Squibb, and Johnson & Johnson; and holds patents, royalties, or other intellectual property rights with Bristol-Myers Squibb. PH additionally reports receiving honoraria from Janssen, Amgen, Karyopharm, Bristol-Myers Squibb, and Sanofi; has been paid for a consultant or advisory role by Janssen, Amgen, Karyopharm, Bristol-Myers Squibb, and Allogen; and received travel, accommodations, and expenses from Johnson & Johnson, Bristol-Myers Squibb, and Sanofi. AS reports honoraria and consulting or advisory role with Iovance Biotherapeutics, Guidepoint, Defined Health, Huron Consulting Group, KeyQuest Health, Istari, Gerson Lehrman Group, Physicians’ Educational Resource, Medscape and MedStar Health; and holds patents, royalties, or other intellectual property rights with Moffitt Cancer Center, Iovance Biotherapeutics, and Provectus.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials