

Trepanation revisited in COVID-19 era: A perspective on craniotomy during current pandemic, surgical technique, and complications avoidance
- PMID: 36600771
- PMCID: PMC9805615
- DOI: 10.25259/SNI_674_2022
Trepanation revisited in COVID-19 era: A perspective on craniotomy during current pandemic, surgical technique, and complications avoidance
Abstract
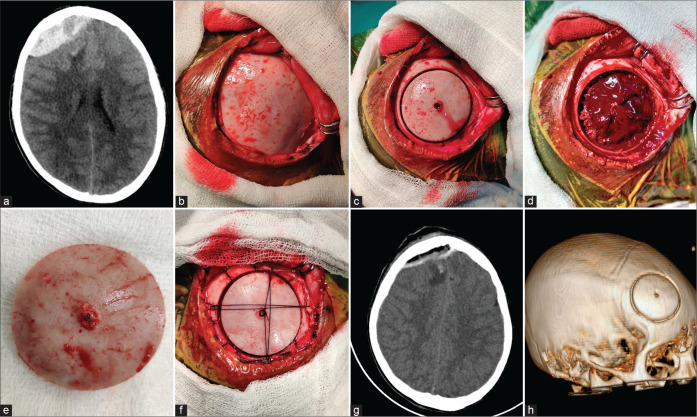
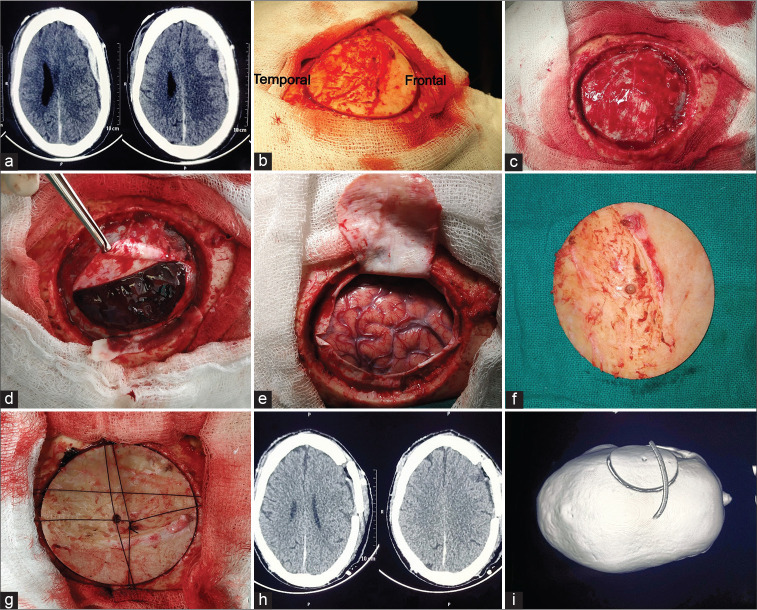
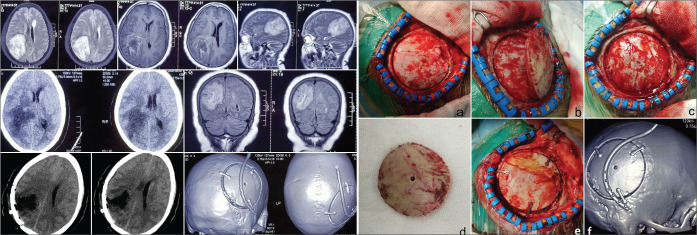
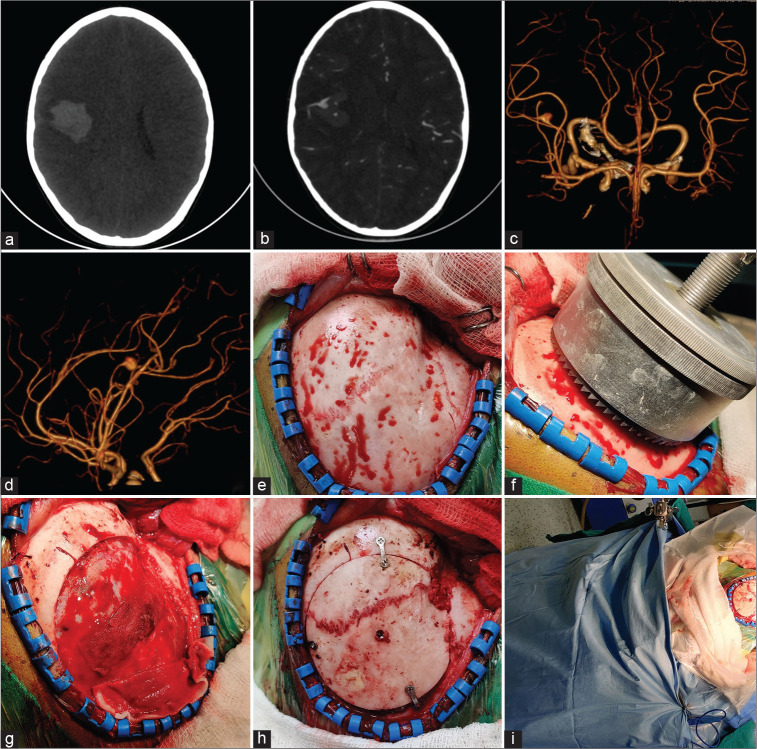
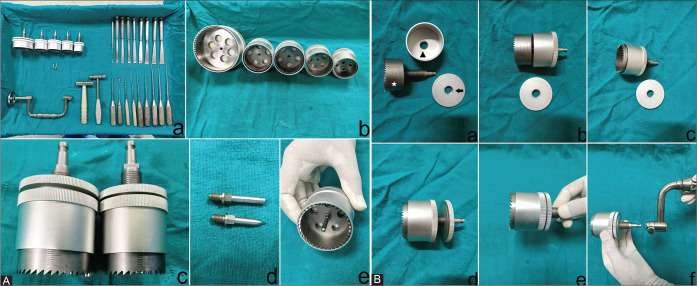
Background: Craniotomy creates maximum aerosols threatening the health care workers (HCWs) of operation room. The technique of trepanation and measures to avoid complications has never been described in the literature. The time taken for craniotomy by different instruments has also never been compared.
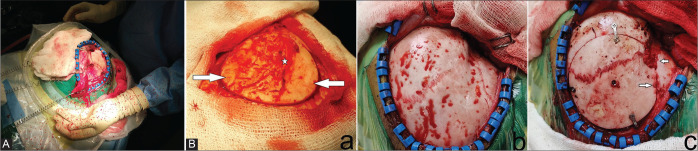
Methods: The study included only COVID-positive patients who underwent surgery. Craniotomy was performed using trephine, pneumatic/power drill (PD), and Hudson brace-Gigli saw (HB-GS). Trepanation as done in 32 patients. The generation of aerosols and time taken for craniotomy by these instruments was observed. The droplet spread over a waterproof graph paper of 10 × 10 sq. cm was calculated in 13 cases of all the three craniotomy methods. The technique of trepanation and maneuvers to overcome complications was discussed.
Results: There was a gross difference in aerosol production and soiling of the surgical drapes, floor, surgeon's glove, gowns, face shield, goggles, etc. The average number of droplet aerosol in trepanation group was 4.76, 23.6 in drill and 21.3 in Gigli saw method. The average time taken for trepanation, PD, and HB-GS craniotomy was 4.8, 22.8, and 24.4 min, respectively. One mortality secondary to COVID was noted. All the HCWs assisting trepanation were negative for COVID-19 during postoperative follow-up of 7 days. However, 13 members of the surgical team which assisted in electric drill and HB-GS methods were COVID-positive.
Conclusion: Trepanation should be the preferred method of craniotomy during COVID-19 pandemic as it is associated with the least aerosolization and is the most time efficient.
Keywords: Aerosol; COVID-19; Craniotomy time; Trepanation; Trephine.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
The authors declare no competing financial interest.
Figures
Similar articles
-
[Secondary decompression trepanation in progressive post-traumatic brain edema after primary decompressive craniotomy].Unfallchirurg. 2003 Oct;106(10):815-25. doi: 10.1007/s00113-003-0663-0. Unfallchirurg. 2003. PMID: 14652724 German.
-
Accidental dural tears occurring during supratentorial craniotomy -- a prospective analysis of predisposing factors in 100 patients.Zentralbl Neurochir. 2005 May;66(2):70-4. doi: 10.1055/s-2005-836476. Zentralbl Neurochir. 2005. PMID: 15846534
-
[Transcranial microsurgical decompression of the optic canal in surgical treatment of meningiomas of the sellar region].Zh Vopr Neirokhir Im N N Burdenko. 2020;84(3):61-73. doi: 10.17116/neiro20208403161. Zh Vopr Neirokhir Im N N Burdenko. 2020. PMID: 32649815 Russian.
-
Guidance for otolaryngology health care workers performing aerosol generating medical procedures during the COVID-19 pandemic.J Otolaryngol Head Neck Surg. 2020 Jun 3;49(1):36. doi: 10.1186/s40463-020-00429-2. J Otolaryngol Head Neck Surg. 2020. PMID: 32493489 Free PMC article. Review.
-
Trepanation in Ancient China.World Neurosurg. 2017 May;101:451-456. doi: 10.1016/j.wneu.2016.10.051. Epub 2016 Oct 18. World Neurosurg. 2017. PMID: 27769950 Review.
References
-
- Beatty RA. Subdural haematomas in the elderly: Experience with treatment by trephine craniotomy and not closing the dura or replacing the bone plate. Br J Neurosurg. 1999;13:60–4. - PubMed
-
- Bynum B, Bynum H. Trepanned cranium. Lancet. 2018;392:112. - PubMed
-
- Chorney MA, Gandhi CD, Prestigiacomo CJ. Berengario’s drill: Origin and inspiration. Neurosurg Focus. 2014;36:E7. - PubMed
-
- Clower WT, Finger S. Discovering trepanation: The contribution of Paul Broca. Neurosurgery. 2001;49:1417–26. - PubMed
-
- González-Darder JM. Cranial trepanation in primitive cultures. Neurocirugia (Astur) 2017;28:28–40. - PubMed
LinkOut - more resources
Full Text Sources