

A Randomized Controlled Trial of Norepinephrine Plus Dobutamine Versus Epinephrine As First-Line Vasoactive Agents in Children With Fluid Refractory Cold Septic Shock
- PMID: 36600781
- PMCID: PMC9799172
- DOI: 10.1097/CCE.0000000000000815
A Randomized Controlled Trial of Norepinephrine Plus Dobutamine Versus Epinephrine As First-Line Vasoactive Agents in Children With Fluid Refractory Cold Septic Shock
Abstract
Our objective was to compare norepinephrine plus dobutamine versus epinephrine as the first-line agent in children with fluid refractory cold septic shock.
Design: Open-label randomized controlled study.
Setting: A single-center PICU from North India.
Patients: Children 2 months to less than 18 years old with fluid refractory cold septic shock.
Interventions: In the intervention group, norepinephrine and dobutamine were started and in the control group, epinephrine was started as the first-line vasoactive agent. The primary outcome was the proportion attaining shock resolution (attaining all the therapeutic endpoints) at 1 hour of therapy.
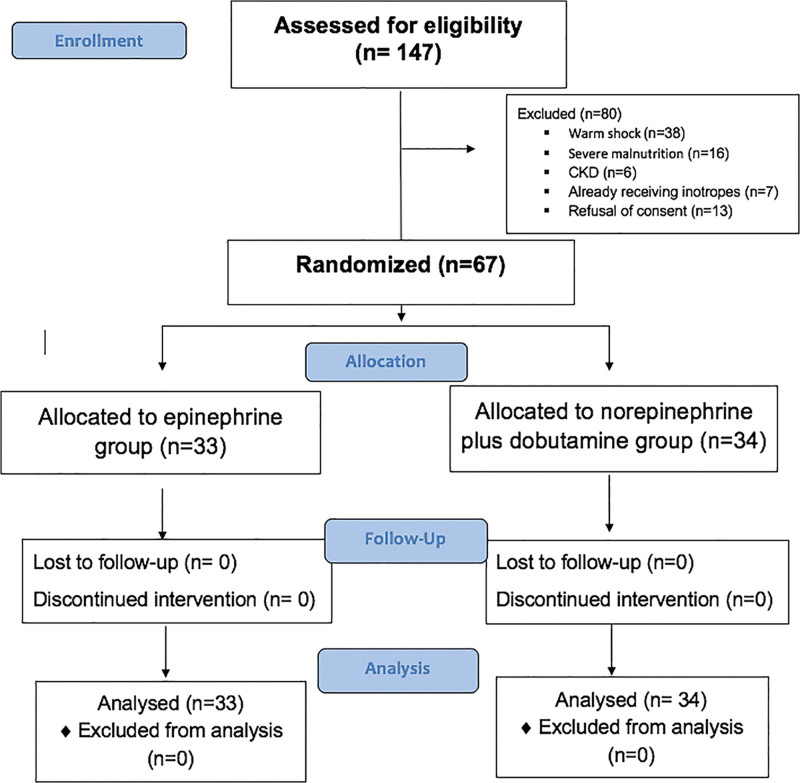
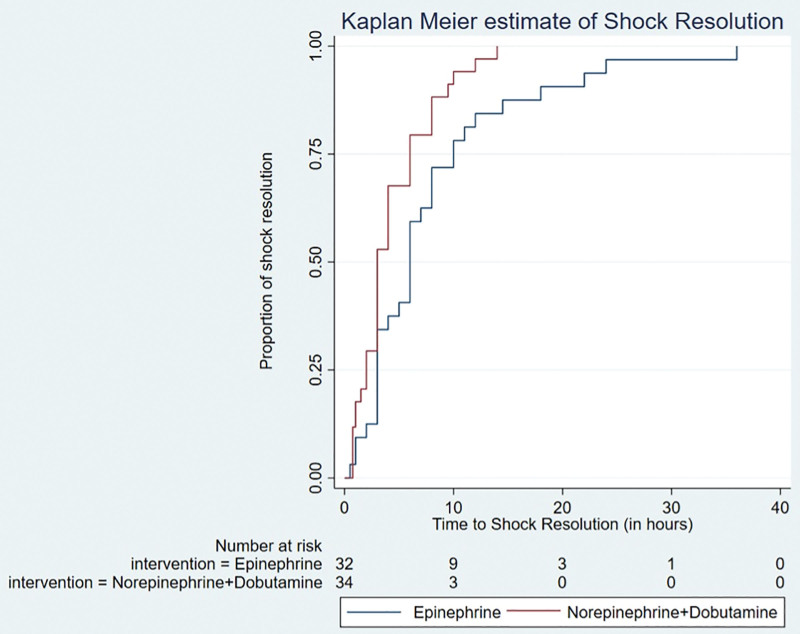
Measurements and main results: We enrolled 67 children: 34 in the norepinephrine plus dobutamine group (intervention) and 33 in the epinephrine group (control). There was no difference in shock resolution at 1 hour (17.6% vs 9%; risk ratio [RR], 2.0; 95% CI, 0.54-7.35; p = 0.25), 6 hours (76.4% vs 54.5%; RR, 1.69; 95% CI, 0.92-3.13; p = 0.06), and 24 hours between the intervention and control groups, respectively. Children in the norepinephrine plus dobutamine group attained shock resolution earlier (measured from starting of vasoactive agents to attaining all the therapeutic endpoints) (hazard ratio, 1.84 [1.1-3.08]). The difference in 28-day mortality was not significant (23.5% vs 39.3% in the intervention and control groups, respectively [RR, 0.59; 95% CI, 0.28-1.25]).
Conclusions: In children with fluid refractory cold septic shock, with use of norepinephrine plus dobutamine as first-line agents, the difference in the proportion of children attaining shock resolution at 1 hour between the groups was inconclusive. However, the time to shock resolution was earlier in the norepinephrine plus dobutamine group. Also, fewer children in the intervention group were refractory to treatment. Further studies powered to detect (or exclude) an important difference would be required to test this intervention.
Keywords: cold; critically ill children; epinephrine; fluid refractory; norepinephrine plus dobutamine; septic shock; vasoconstricted shock.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Davis AL, Carcillo JA, Aneja RK, et al. : American College of Critical Care Medicine clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock. Crit Care Med 2017; 45:1061–1093 - PubMed
-
- Ceneviva G, Paschall JA, Maffei F, et al. : Hemodynamic support in fluid- refractory pediatric septic shock. Pediatrics 1998; 102:e19. - PubMed
-
- Dalimonte MA, DeGrado JR, Anger KE: Vasoactive agents for adult septic shock: An update and review. J Pharm Pract 2020; 33:523–532 - PubMed
-
- Ranjit S, Aram G, Kissoon N, et al. : Multimodal monitoring for hemodynamic categorization and management of pediatric septic shock: A pilot observational study. Pediatr Crit Care Med 2014; 15:e17–e26 - PubMed
-
- Brierley J, Peters MJ: Distinct hemodynamic patterns of septic shock at presentation to pediatric intensive care. Pediatrics 2008; 122:752–759 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
