

Outcomes of Patients with Advanced Urothelial Carcinoma after Anti-programmed Death-(ligand) 1 Therapy by Fibroblast Growth Factor Receptor Gene Alteration Status: An Observational Study
- PMID: 36601039
- PMCID: PMC9806713
- DOI: 10.1016/j.euros.2022.11.001
Outcomes of Patients with Advanced Urothelial Carcinoma after Anti-programmed Death-(ligand) 1 Therapy by Fibroblast Growth Factor Receptor Gene Alteration Status: An Observational Study
Abstract
Background: Clinical outcomes of anti-programmed death‑(ligand) 1 (anti-PD-[L]1) therapy in patients with locally advanced or metastatic urothelial carcinoma (mUC) and fibroblast growth factor receptor alterations (FGFRa+) remain unclear; recent studies have reported either comparable or poorer outcomes versus patients without FGFR alterations (FGFRa-).
Objective: To analyze the outcomes of patients with mUC and any FGFRa (mutations or fusions) who received anti-PD-(L)1 therapy.
Design setting and participants: In this noninterventional, retrospective, multicenter study, clinical practice data were collected from FGFRa+/- patients who received prior immunotherapy between May 2018 and July 2019.
Outcome measurements and statistical analysis: Investigator‑determined overall response rate (ORR), disease control rate (DCR), and overall survival (OS) were assessed in multivariate and unadjusted analyses.
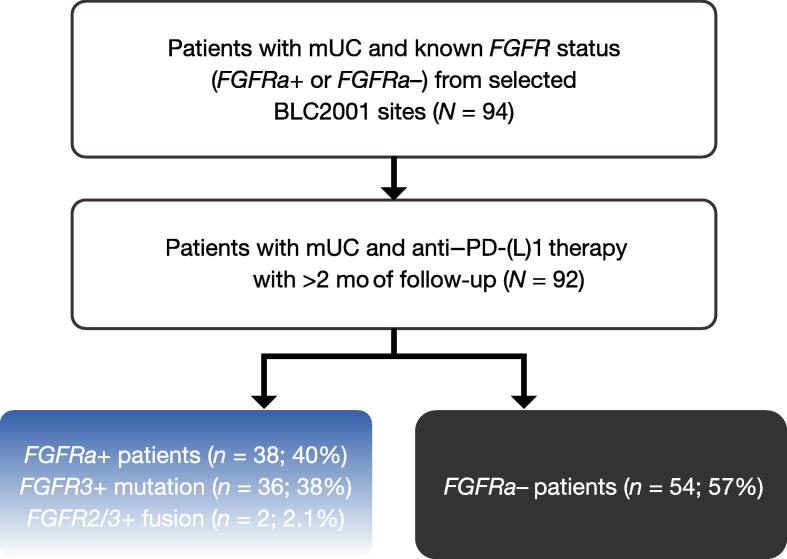
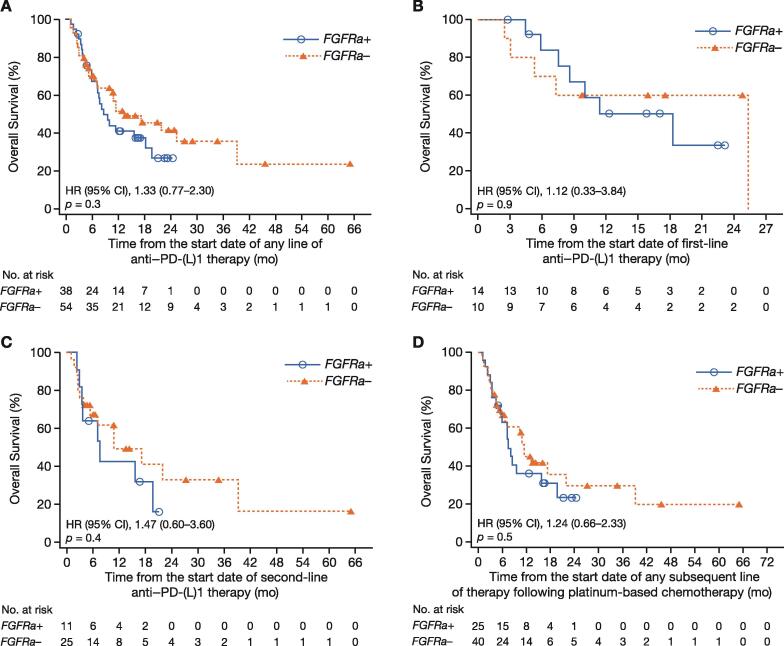
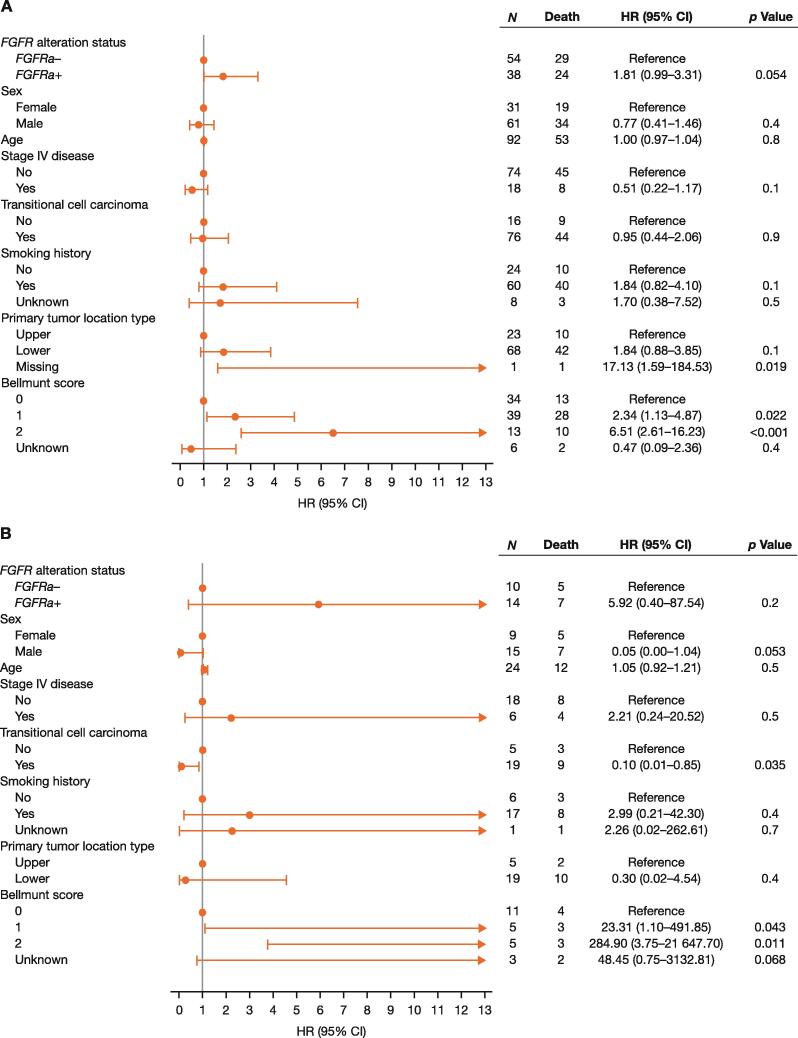
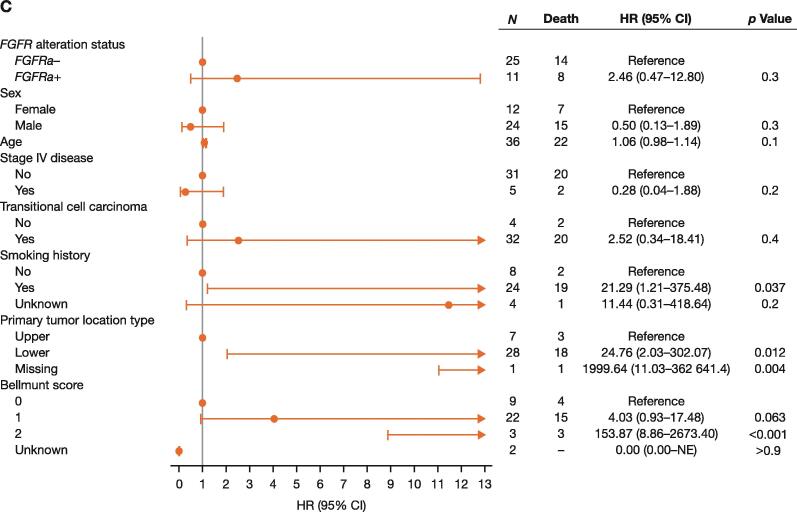
Results and limitations: Ninety-four patients (66% men; median age, 63 yr) with mUC and known FGFR status were included; 38 (40%) were FGFRa+ and 56 (60%) were FGFRa-. In FGFRa+ versus FGFRa- patients who received any line of anti-PD-(L)1 therapy (n = 92), ORR, DCR, and OS were 16% versus 26%, 29% versus 52% (relative risk: 1.14 [95% confidence interval {CI}, 0.92-1.40]; p = 0.3), and 8.57 versus 13.2 mo (hazard ratio [HR]: 1.33 [95% CI, 0.77-2.30]; p = 0.3), respectively. A multivariate analysis provided some evidence supporting shorter OS in FGFRa+ versus FGFRa- (any line of anti-PD-L[1] therapy; HR: 1.81 [95% CI, 0.99-3.31]; p = 0.054). Limitations include this study's retrospective nature and a potential selection bias from small sample size.
Conclusions: Some evidence of lower response rates and shortened OS following anti-PD-(L)1 therapy was observed in FGFRa+ patients. The phase 3 THOR study (NCT03390504) will prospectively compare FGFRa+ patients with advanced mUC treated with erdafitinib versus pembrolizumab.
Patient summary: Patients with metastatic urothelial carcinoma and prespecified fibroblast growth factor receptor alterations (FGFRa) potentially have worse clinical outcomes when treated with anti-PD-(L)1 therapy than those without FGFRa.
Keywords: Anti–programmed death-(ligand) 1 therapy; FGFR alteration; Fibroblast growth factor receptor; Programmed cell death protein 1; Programmed death-(ligand) 1; Urothelial carcinoma.
© 2022 The Authors.
Figures
References
-
- KEYTRUDA [prescribing information]. Whitehouse Station, NJ: Merck Sharp & Dohme Corp; 2021.
-
- TECENTRIQ [prescribing information]. South San Francisco, CA: Genentech, Inc.; 2019.
-
- OPDIVO [prescribing information]. Princeton, NJ: Bristol-Myers Squibb Company; 2022.
-
- BAVENCIO [prescribing information]. Darmstadt, Germany: Merck KGaA; 2017.
-
- van der Heijden M.S., Loriot Y., Duran I., et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma: a long-term overall survival and safety update from the phase 3 IMvigor211 clinical trial. Eur Urol. 2021;80:7–11. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
