

Positioning the Catheter Tip Anterior or Posterior to the Saphenous Nerve in Continuous Adductor Canal Block: A Mono-Centric Retrospective Comparative Study
- PMID: 36601486
- PMCID: PMC9807124
- DOI: 10.2147/LRA.S383601
Positioning the Catheter Tip Anterior or Posterior to the Saphenous Nerve in Continuous Adductor Canal Block: A Mono-Centric Retrospective Comparative Study
Abstract
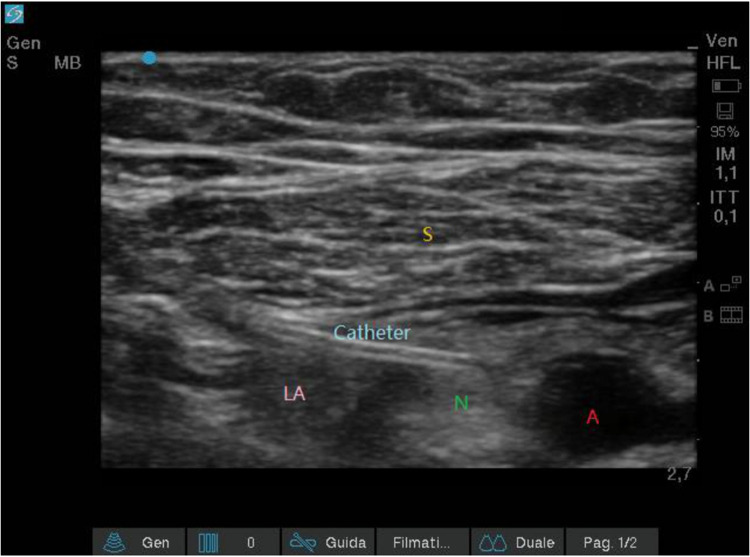
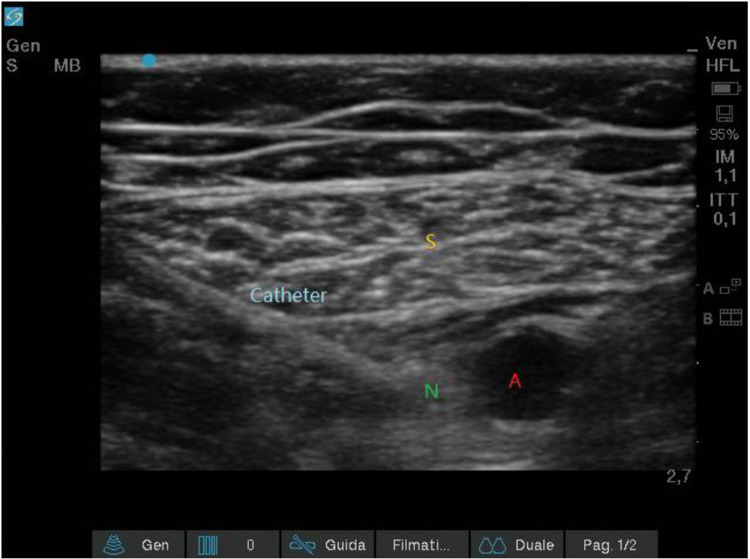
Background and aim: Ultrasound-guided continuous adductor canal block (cACB) is a conventional choice in patients undergoing total knee arthroplasty (TKA) for the management of the postoperative pain. This study aims to compare different catheter tip locations for cACB relative to the saphenous nerve (anteriorly vs posteriorly) in terms of efficacy and complications.
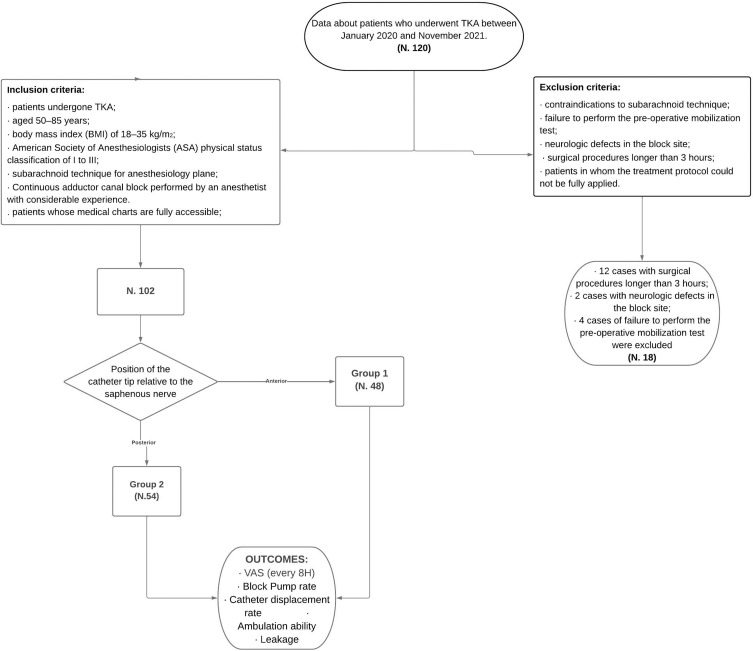
Methods: At the department of Surgical Sciences, Orthopedic Trauma and Emergencies of the University of Naples Federico II (Naples, Italy), between January 2020 and November 2021, retrospective comparative study was executed. Patients planned for TKA were included in the study if they met the follow inclusion criteria: patients undergone TKA; aged 50-85 years; body mass index (BMI) of 18-35 kg/m2; American Society of Anesthesiologists (ASA) physical status classification from I to III; subarachnoid technique for anesthesiology plane; continuous adductor canal block performed by an anesthetist with considerable experience. Patients were assigned to receive cACB with the catheter tip located anteriorly (Group 1, G1) or posteriorly to the saphenous nerve (Group 2, G2). Postoperative pain, ambulation ability, episodes of pump block and rate of catheter dislodgement and leakage were evaluated and analyzed.
Results: Altogether, 102 patients were admitted to the study (48 in G1 and 54 in G2). After the first 8 postoperative hours, in G1 17 patients (35.4%) had a VAS greater than 4, while in group 2 only 3 patients (5.6%) had a VAS greater than 4 (p-value <0.01). All patients of both groups showed ambulation ability in the postoperative period. No episode of leakage was recorded. While the catheter displacement rate was similar in the two groups (2.1% for G1 vs 3.7% for G2; p-value >0.05), the episodes of pump block were significantly less in G2 than in G1 (3.7% vs 20.8%; p-value <0.01).
Conclusion: In cACB for TKA, we found that positioning the catheter tip posteriorly to the saphenous nerve may lead to a greater postoperative analgesia and reduce the risk of pump block compared to placing the catheter tip anteriorly to the nerve.
Keywords: catheter displacement; catheter location; continuous adductor canal block; saphenous nerve; total knee arthroplasty.
© 2022 Coviello et al.
Conflict of interest statement
The authors declare no competing interests in this work.
Figures
Similar articles
-
The effect of continuous adductor canal block combined with distal interspace between the popliteal artery and capsule of the posterior knee block for total knee arthroplasty: a randomized, double-blind, controlled trial.BMC Anesthesiol. 2022 Jun 6;22(1):175. doi: 10.1186/s12871-022-01712-7. BMC Anesthesiol. 2022. PMID: 35668348 Free PMC article. Clinical Trial.
-
Continuous adductor canal block is superior to adductor canal block alone or adductor canal block combined with IPACK block (interspace between the popliteal artery and the posterior capsule of knee) in postoperative analgesia and ambulation following total knee arthroplasty: randomized control trial.Musculoskelet Surg. 2022 Jun;106(2):155-162. doi: 10.1007/s12306-020-00682-8. Epub 2020 Sep 27. Musculoskelet Surg. 2022. PMID: 32980982 Clinical Trial.
-
Postoperative continuous adductor canal block for total knee arthroplasty improves pain and functional recovery: A randomized controlled clinical trial.J Clin Anesth. 2018 Sep;49:46-52. doi: 10.1016/j.jclinane.2018.06.004. Epub 2018 Jun 8. J Clin Anesth. 2018. PMID: 29890381 Clinical Trial.
-
Is continuous catheter adductor canal block better than single-shot canal adductor canal block in primary total knee arthroplasty?: A GRADE analysis of the evidence through a systematic review and meta-analysis.Medicine (Baltimore). 2020 May;99(20):e20320. doi: 10.1097/MD.0000000000020320. Medicine (Baltimore). 2020. PMID: 32443383 Free PMC article.
-
The Efficacy and Safety of Regional Nerve Blocks in Total Knee Arthroplasty: Systematic Review and Direct Meta-Analysis.J Arthroplasty. 2022 Oct;37(10):1906-1921.e2. doi: 10.1016/j.arth.2022.03.078. J Arthroplasty. 2022. PMID: 36162923
Cited by
-
Dexamethasone versus Dexmedetomidine as Adjuvants in Ultrasound Popliteal Sciatic Nerve Block for Hallux Valgus Surgery: A Mono-Centric Retrospective Comparative Study.Drug Des Devel Ther. 2024 Apr 17;18:1231-1245. doi: 10.2147/DDDT.S442808. eCollection 2024. Drug Des Devel Ther. 2024. PMID: 38645991 Free PMC article.
-
The Twenty-Five Most Cited Articles About Adductor Canal Block: A Bibliometric Analysis from 1980 to 2022.J Pain Res. 2023 Oct 2;16:3353-3365. doi: 10.2147/JPR.S415184. eCollection 2023. J Pain Res. 2023. PMID: 37808463 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
