

Pembrolizumab induced remission of recurrent and metastatic sinonasal squamous cell carcinoma after overcoming checkpoint-inhibitor pneumonitis: A case report and literature review
- PMID: 36601913
- PMCID: PMC10363840
- DOI: 10.1002/cnr2.1778
Pembrolizumab induced remission of recurrent and metastatic sinonasal squamous cell carcinoma after overcoming checkpoint-inhibitor pneumonitis: A case report and literature review
Abstract
Background: For programmed death-ligand-1 (PD-L1) positive recurrent and metastatic head and neck squamous cell carcinoma (R/M-HNSCC), KEYNOTE-048 and KEYNOTE-040 clinical trials recently approved pembrolizumab monotherapy as first-line treatment. However, recurrent and metastatic sinonasal squamous cell carcinoma (R/M-SNSCC) was excluded from these clinical trials and treatment reports of immune-checkpoint inhibitor (ICI) in R/M-SNSCC are sparse. Immune-related adverse events (irAEs) are known to occur during ICI treatment and some of these such as checkpoint-inhibitor pneumonitis (CIP) can be fatal. ICI rechallenge after severe irAEs is debated.
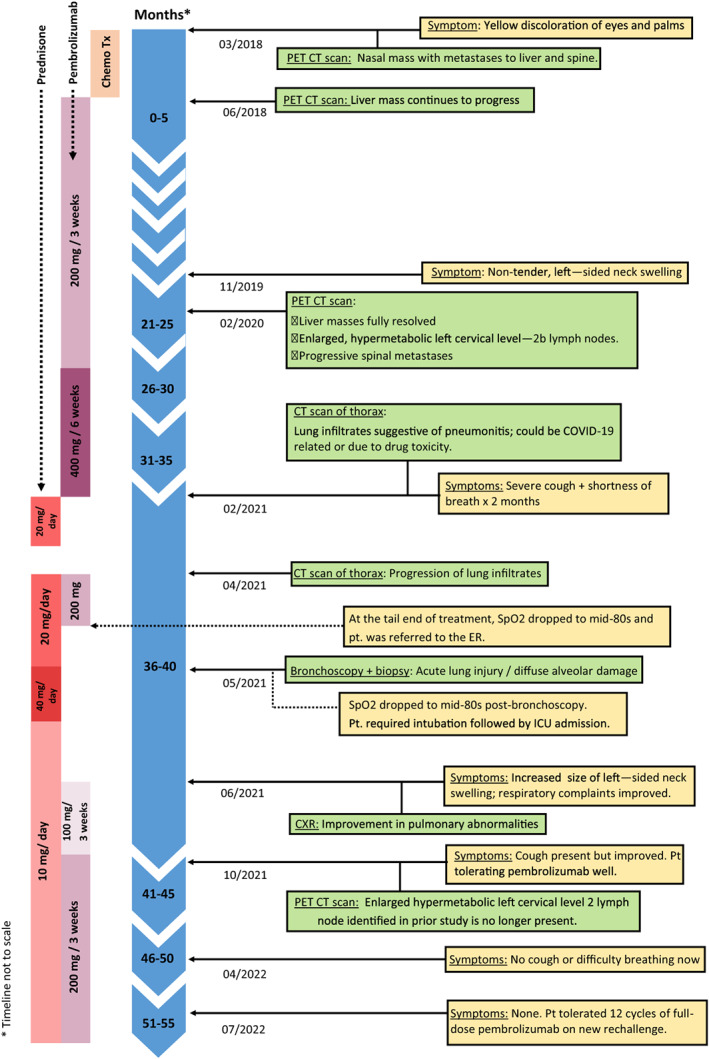
Case: We describe a case of a 65-year-old male with R/M-SNSCC who is currently in remission with pembrolizumab monotherapy. He developed high-grade pneumonitis during the course of treatment warranting ICI discontinuation but has since tolerated full-dose pembrolizumab for 10 months now which is holding his disease stable. Our approach toward restarting full-dose pembrolizumab was by monitoring the patient's response to an initial low dose of pembrolizumab with concomitant oral steroid immunosuppression to control CIP.
Conclusion: Clinicians should weigh the risk-to-reward ratio of ICI rechallenge after improvement of high-grade CIP, particularly for selected patients with aggressive tumors such as R/M-SNSCC and prior treatment response. Under close monitoring, ICI resumption at a low dose and assessing patient tolerance with concomitant immunosuppression may be a reasonable approach to reintroducing ICI after high-grade CIP in these patients.
Keywords: checkpoint-inhibitor pneumonitis; immunotherapy; pembrolizumab; sinonasal squamous cell carcinoma.
© 2023 The Authors. Cancer Reports published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Dutta R, Dubal PM, Svider PF, Liu JK, Baredes S, Eloy JA. Sinonasal malignancies: A population‐based analysis of site‐specific incidence and survival. Laryngoscope. 2015;125(11):2491‐2497. - PubMed
-
- Mahalingappa YB, Khalil HS. Sinonasal malignancy: presentation and outcomes. J Laryngol Otol. 2014;128(7):654‐657. - PubMed
-
- Cohen EEW, Soulières D, le Tourneau C, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head‐and‐neck squamous cell carcinoma (KEYNOTE‐040): a randomised, open‐label, phase 3 study. Lancet. 2019;393(10167):156‐167. - PubMed
-
- Burtness B, Harrington KJ, Greil R, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE‐048): a randomised, open‐label, phase 3 study. Lancet. 2019;394(10212):1915‐1928. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
