

HRAS Mutations Define a Distinct Subgroup in Head and Neck Squamous Cell Carcinoma
- PMID: 36603172
- PMCID: PMC9928766
- DOI: 10.1200/PO.22.00211
HRAS Mutations Define a Distinct Subgroup in Head and Neck Squamous Cell Carcinoma
Abstract
Purpose: In head and neck squamous cell carcinoma (HNSCC), HRAS mutation is a new actionable oncogene driver. We aimed to evaluate HRAS mutational variants, comutation profile, and survival outcomes of this molecularly defined population.
Methods: We leveraged four deidentified patient data sets with HRAS-mutant HNSCC, MD Anderson Cancer Center, Kura Oncology, Inc trial, Foundation Medicine, and American Association for Cancer Research GENIE v.12. Patient demographic information and clinical courses were extracted, when available, in addition to HRAS mutation type and co-occurring mutations. Survival outcomes were analyzed (Kaplan-Meier method).
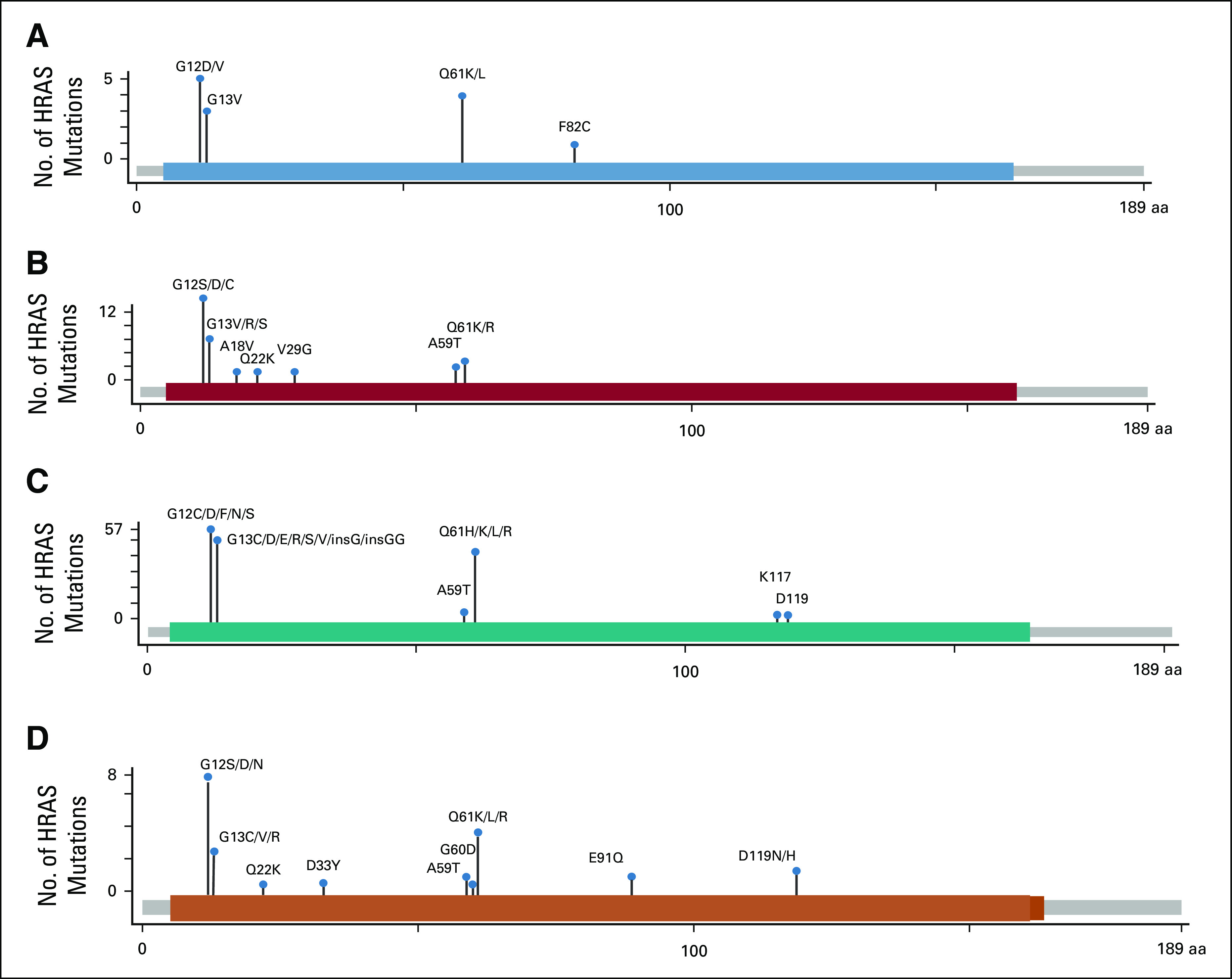
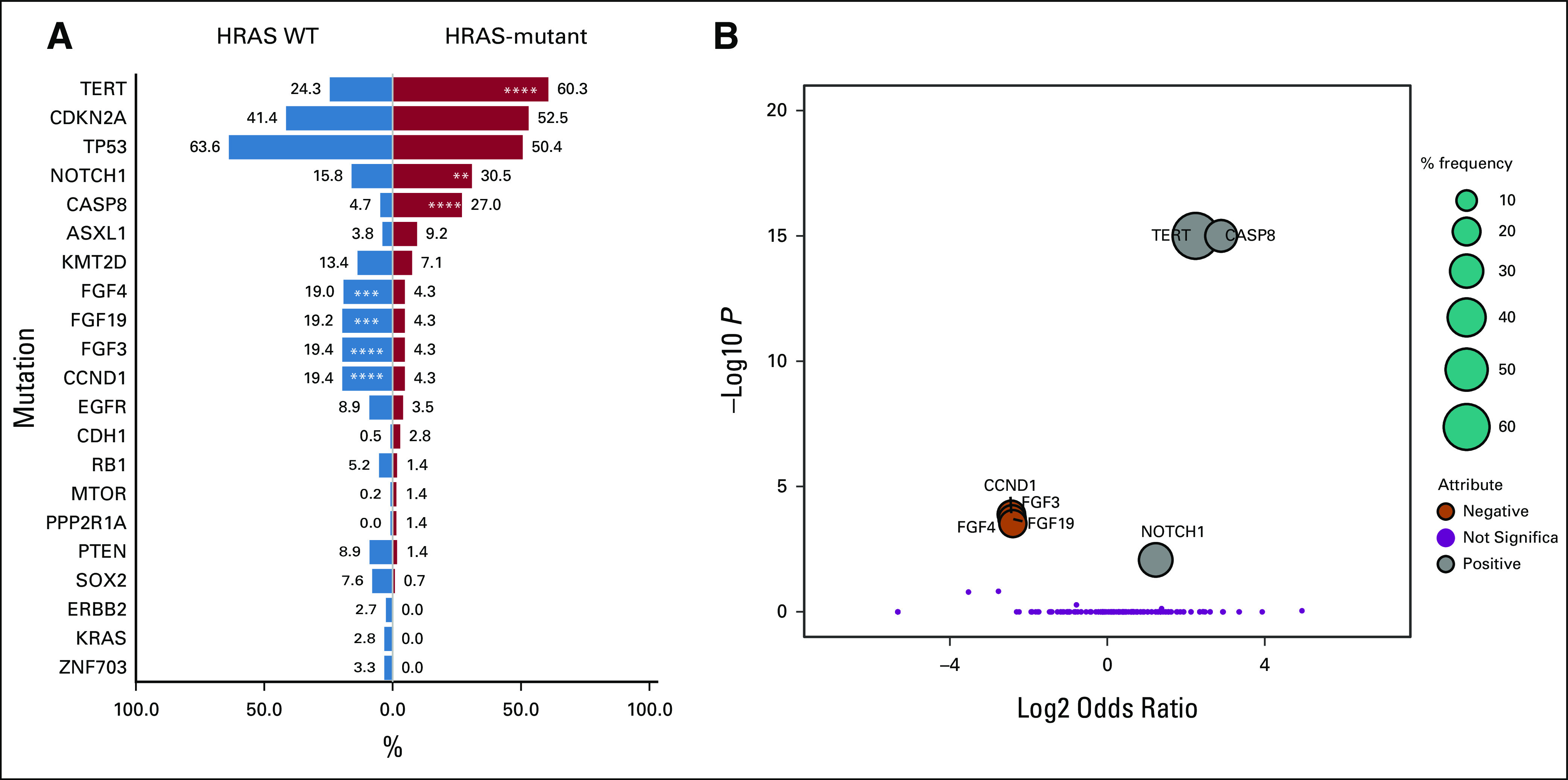
Results: Two hundred forty-nine patients with HRAS-mutant HNSCC were identified from the four data sets. Median age ranged from 55 to 65 years, with a higher frequency in male patients (64%); the majority of HRAS-mutant HNSCC occurred in human papillomavirus-negative HNSCC. HRAS mutation patterns were similar across data sets; G12S was the most common (29%). Treatment responses to tipifarnib were not codon-specific. Compared with wild-type, significantly co-occurring mutations with HRAS were Casp8 (Fisher's exact test, P < .00013), TERT (P < .0085), and NOTCH1 (P < .00013). Analysis of clinical courses from the MD Anderson Cancer Center and Kura Oncology, Inc data sets demonstrated poor clinical outcomes with a high rate of recurrence following primary definitive treatment (50%-67% relapse < 6 months) and short disease-free survival (4.0 months; 95% CI, 1.0 to 36.0) and overall survival (OS; 15.0 months; 95% CI, 6.0 to 52.0). Use of tipifarnib in this data set demonstrated improved OS (25.5 months; 95% CI, 18.0 to 48.0).
Conclusion: Oncogenic mutations in HRAS occur in 3%-4% of HNSCC, with G12S being the most frequent. Without targeted therapy, patients with HRAS-mutant HNSCC had poor clinic outcomes; observable trend toward improvement in OS has been noted in cohorts receiving treatments such as tipifarnib. The comutation pattern of HRAS-mutant in HNSCC is distinct, which may provide insight to future therapeutic combination strategies.
Conflict of interest statement
No other potential conflicts of interest were reported.
Figures



Similar articles
-
Evolutionary dynamics of tipifarnib in HRAS mutated head and neck squamous cell carcinoma.Oral Oncol. 2024 Feb;149:106688. doi: 10.1016/j.oraloncology.2024.106688. Epub 2024 Jan 13. Oral Oncol. 2024. PMID: 38219706 Free PMC article.
-
Tipifarnib in Head and Neck Squamous Cell Carcinoma With HRAS Mutations.J Clin Oncol. 2021 Jun 10;39(17):1856-1864. doi: 10.1200/JCO.20.02903. Epub 2021 Mar 22. J Clin Oncol. 2021. PMID: 33750196 Free PMC article. Clinical Trial.
-
Concurrent Inhibition of ERK and Farnesyltransferase Suppresses the Growth of HRAS Mutant Head and Neck Squamous Cell Carcinoma.Mol Cancer Ther. 2022 May 4;21(5):762-774. doi: 10.1158/1535-7163.MCT-21-0142. Mol Cancer Ther. 2022. PMID: 35247914 Free PMC article.
-
Mutant HRas Signaling and Rationale for Use of Farnesyltransferase Inhibitors in Head and Neck Squamous Cell Carcinoma.Target Oncol. 2023 Sep;18(5):643-655. doi: 10.1007/s11523-023-00993-3. Epub 2023 Sep 4. Target Oncol. 2023. PMID: 37665491 Review.
-
Targeting Harvey rat sarcoma viral oncogene homolog in head and neck cancer: how to move forward?Curr Opin Oncol. 2023 May 1;35(3):178-185. doi: 10.1097/CCO.0000000000000943. Epub 2023 Mar 17. Curr Opin Oncol. 2023. PMID: 36966498 Review.
Cited by
-
The immunologic landscape of HRAS-mutant head and neck squamous-cell carcinoma.ESMO Open. 2025 Aug;10(8):105538. doi: 10.1016/j.esmoop.2025.105538. Epub 2025 Aug 12. ESMO Open. 2025. PMID: 40803018 Free PMC article.
-
Molecular Mechanisms in the Carcinogenesis of Oral Squamous Cell Carcinoma: A Literature Review.Biomolecules. 2025 Apr 25;15(5):621. doi: 10.3390/biom15050621. Biomolecules. 2025. PMID: 40427514 Free PMC article. Review.
-
Advanced Human Papillomavirus-Negative Head and Neck Squamous Cell Carcinoma: Unmet Need and Emerging Therapies.Mol Cancer Ther. 2024 Dec 3;23(12):1717-1730. doi: 10.1158/1535-7163.MCT-24-0281. Mol Cancer Ther. 2024. PMID: 39301607 Free PMC article. Review.
-
Farnesyl-transferase inhibitors show synergistic anticancer effects in combination with novel KRAS-G12C inhibitors.Br J Cancer. 2024 Apr;130(6):1059-1072. doi: 10.1038/s41416-024-02586-x. Epub 2024 Jan 26. Br J Cancer. 2024. PMID: 38278976 Free PMC article.
-
Evolutionary dynamics of tipifarnib in HRAS mutated head and neck squamous cell carcinoma.Oral Oncol. 2024 Feb;149:106688. doi: 10.1016/j.oraloncology.2024.106688. Epub 2024 Jan 13. Oral Oncol. 2024. PMID: 38219706 Free PMC article.
References
-
- Sklan A, Collingridge D: Treating head and neck cancer: For better or for worse? Lancet Oncol 18:570-571, 2017 - PubMed
-
- Burtness B, Harrington KJ, Greil R, et al. : Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 394:1915-1928, 2019 - PubMed
-
- Li S, Balmain A, Counter CM: A model for RAS mutation patterns in cancers: Finding the sweet spot. Nat Rev Cancer 18:767-777, 2018 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
