

Multicenter Phase II Clinical Trial of Gemcitabine and Cisplatin as Neoadjuvant Chemotherapy for Patients With High-Grade Upper Tract Urothelial Carcinoma
- PMID: 36603175
- PMCID: PMC10043554
- DOI: 10.1200/JCO.22.00763
Multicenter Phase II Clinical Trial of Gemcitabine and Cisplatin as Neoadjuvant Chemotherapy for Patients With High-Grade Upper Tract Urothelial Carcinoma
Abstract
Purpose: Neoadjuvant chemotherapy (NAC) has proven survival benefits for patients with invasive urothelial carcinoma of the bladder, yet its role for upper tract urothelial carcinoma (UTUC) remains undefined. We conducted a multicenter, single-arm, phase II trial of NAC with gemcitabine and split-dose cisplatin (GC) for patients with high-risk UTUC before extirpative surgery to evaluate response, survival, and tolerability.
Methods: Eligible patients with defined criteria for high-risk localized UTUC received four cycles of split-dose GC before surgical resection and lymph node dissection. The primary study end point was rate of pathologic response (defined as < ypT2N0). Secondary end points included progression-free survival (PFS), overall survival (OS), and safety and tolerability.
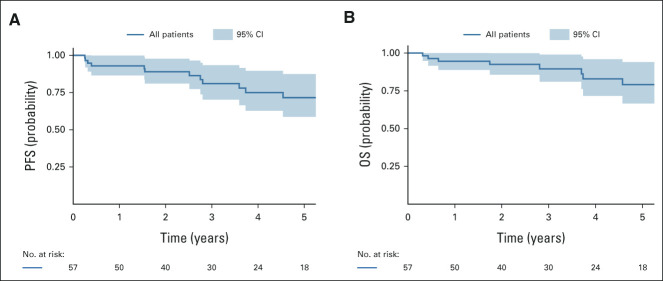
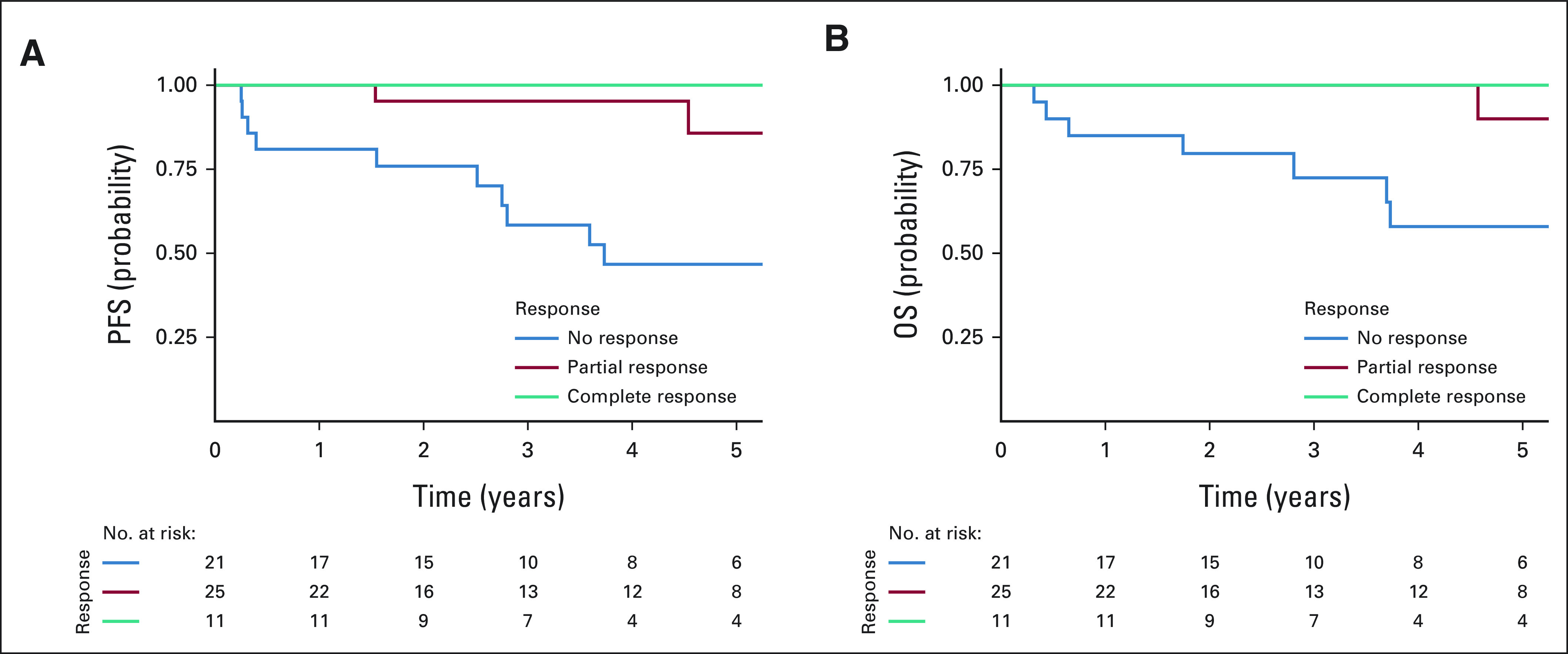
Results: Among 57 patients evaluated, 36 (63%) demonstrated pathologic response (95% CI, 49 to 76). A complete pathologic response (ypT0N0) was noted in 11 patients (19%). Fifty-one patients (89%) tolerated at least three complete cycles of split-dose GC, 27 patients (47%) tolerated four complete cycles, and all patients proceeded to surgery. With a median follow up of 3.1 years, 2- and 5-year PFS rates were 89% (95% CI, 81 to 98) and 72% (95% CI, 59 to 87), while 2- and 5-year OS rates were 93% (95% CI, 86 to 100) and 79% (95% CI, 67 to 94), respectively. Pathologic complete and partial responses were associated with improved PFS and OS compared with nonresponders (≥ ypT2N any; 2-year PFS 100% and 95% v 76%, P < .001; 2-year OS 100% and 100% v 80%, P < .001).
Conclusion: NAC with split-dose GC for high-risk UTUC is a well-tolerated, effective therapy demonstrating evidence of pathologic response that is associated with favorable survival outcomes. Given that these survival outcomes are superior to historical series, these data support the use of NAC as a standard of care for high-risk UTUC, and split-dose GC is a viable option for NAC.
Trial registration: ClinicalTrials.gov NCT01261728.
Conflict of interest statement
Multicenter Phase II Clinical Trial of Gemcitabine and Cisplatin as Neoadjuvant Chemotherapy for Patients With High-Grade Upper Tract Urothelial Carcinoma
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures
References
-
- Munoz JJ, Ellison LM. Upper tract urothelial neoplasms: Incidence and survival during the last 2 decades. J Urol. 2000;164:1523–1525. - PubMed
-
- Collà Ruvolo C, Nocera L, Stolzenbach LF, et al. Incidence and survival rates of contemporary patients with invasive upper tract urothelial carcinoma. Eur Urol Oncol. 2021;4:792–801. - PubMed
-
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349:859–866. - PubMed
-
- Collaboration ABCAM-a. Neoadjuvant chemotherapy in invasive bladder cancer: Update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur Urol. 2005;48:202–205. discussion 5-6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
