

Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2019
- PMID: 36603845
- PMCID: PMC10062373
- DOI: 10.1093/europace/euac237
Global burden of atrial fibrillation/atrial flutter and its attributable risk factors from 1990 to 2019
Abstract
Aims: The aim of this study was to estimate the global burden of atrial fibrillation (AF)/atrial flutter (AFL) and its attributable risk factors from 1990 to 2019.
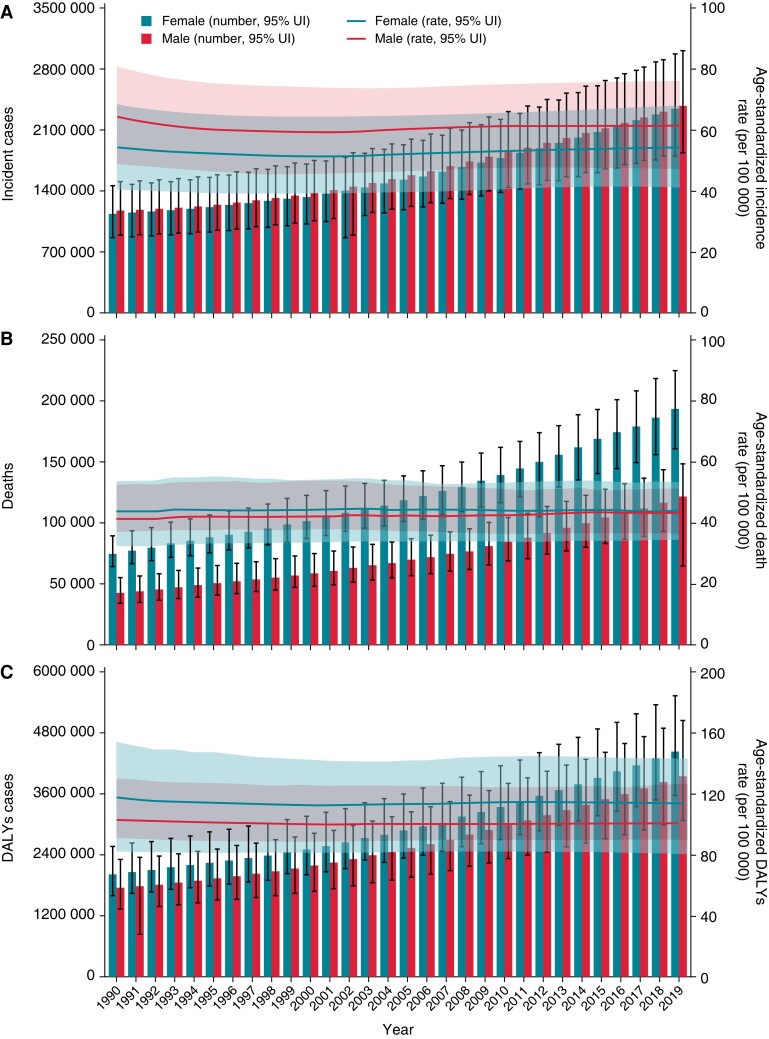
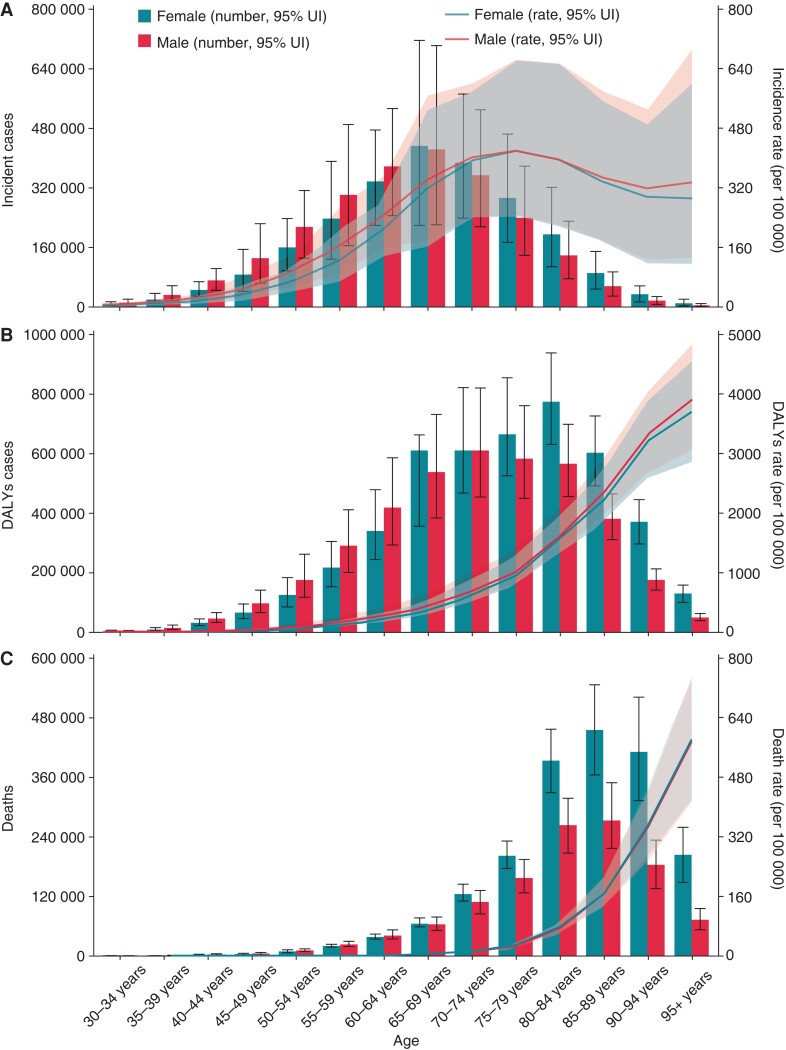
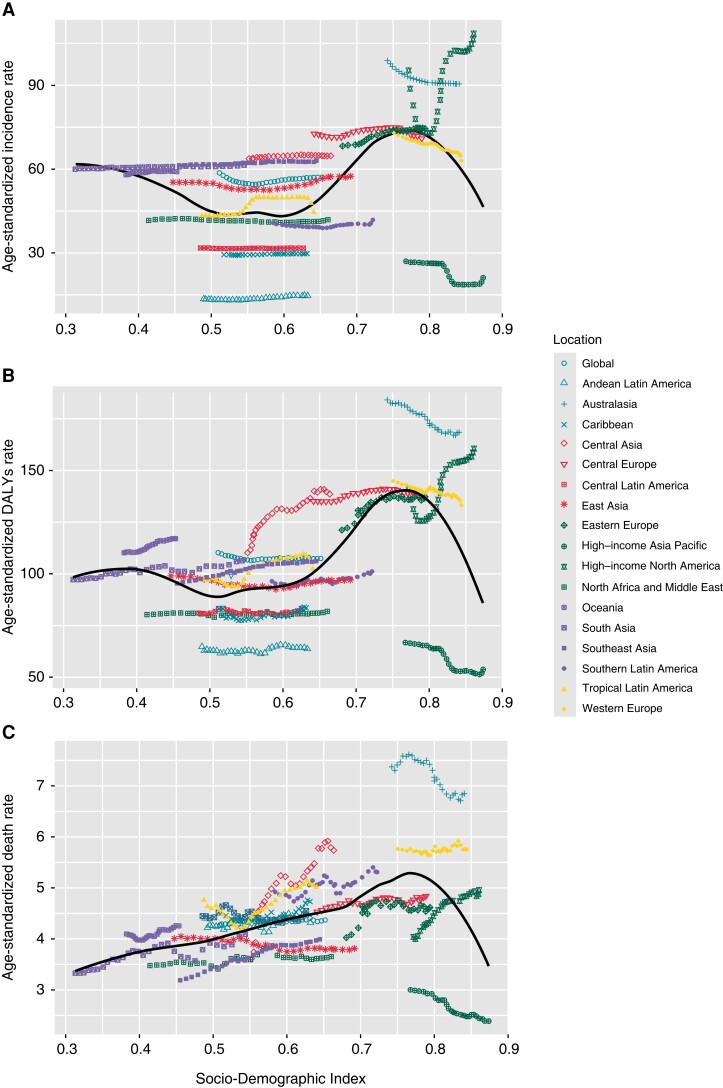
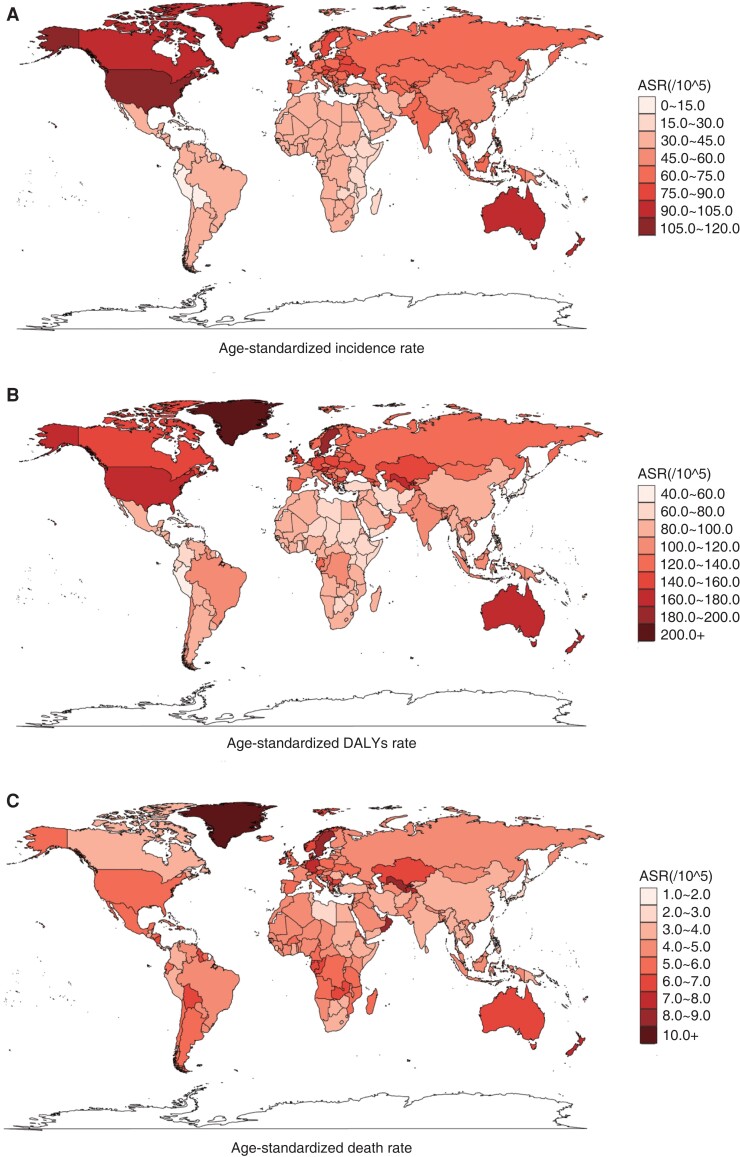
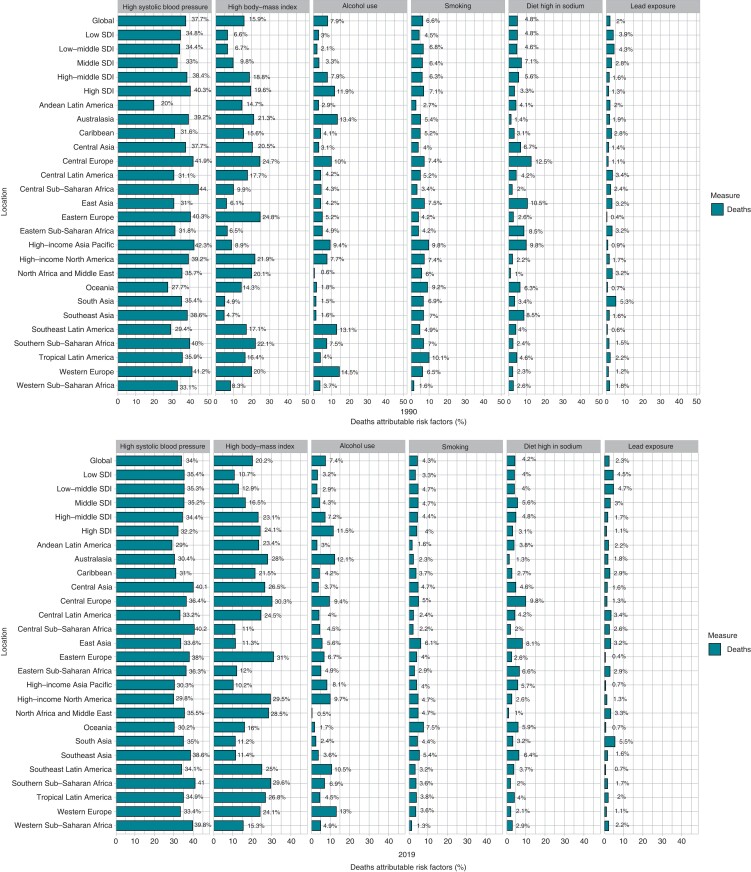
Methods and results: The data on AF/AFL were retrieved from the Global Burden of Disease Study (GBD) 2019. Incidence, disability-adjusted life years (DALYs), and deaths were metrics used to measure AF/AFL burden. The population attributable fractions (PAFs) were used to calculate the percentage contributions of major potential risk factors to age-standardized AF/AFL death. The analysis was performed between 1990 and 2019. Globally, in 2019, there were 4.7 million [95% uncertainty interval (UI): 3.6 to 6.0] incident cases, 8.4 million (95% UI: 6.7 to 10.5) DALYs cases, and 0.32 million (95% UI: 0.27 to 0.36) deaths of AF/AFL. The burden of AF/AFL in 2019 and their temporal trends from 1990 to 2019 varied widely due to gender, Socio-Demographic Index (SDI) quintile, and geographical location. Among all potential risk factors, age-standardized AF/AFL death worldwide in 2019 were primarily attributable to high systolic blood pressure [34.0% (95% UI: 27.3 to 41.0)], followed by high body mass index [20.2% (95% UI: 11.2 to 31.2)], alcohol use [7.4% (95% UI: 5.8 to 9.0)], smoking [4.3% (95% UI: 2.9 to 5.9)], diet high in sodium [4.2% (95% UI: 0.8 to 10.5)], and lead exposure [2.3% (95% UI: 1.3 to 3.4)].
Conclusion: Our study showed that AF/AFL is still a major public health concern. Despite the advancements in the prevention and treatment of AF/AFL, especially in regions in the relatively SDI quintile, the burden of AF/AFL in regions in lower SDI quintile is increasing. Since AF/AFL is largely preventable and treatable, there is an urgent need to implement more cost-effective strategies and interventions to address modifiable risk factors, especially in regions with high or increased AF/AFL burden.
Keywords: Atrial fibrillation/atrial flutter; Deaths; Disability-adjusted life years; Global burden; Incidence; Risk factors.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Stewart S, Hart C, Hole D, McMurray J. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med 2002;113:359–64. - PubMed
-
- Wang L, Ze F, Li J, Mi L, Han B, Niu H. Trends of global burden of atrial fibrillation/flutter from Global Burden of Disease Study 2017. Heart 2021;107:881–7. - PubMed
-
- Naccarelli G, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol 2009;104:1534–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
