

T cell receptor repertoires associated with control and disease progression following Mycobacterium tuberculosis infection
- PMID: 36604540
- PMCID: PMC9873565
- DOI: 10.1038/s41591-022-02110-9
T cell receptor repertoires associated with control and disease progression following Mycobacterium tuberculosis infection
Abstract
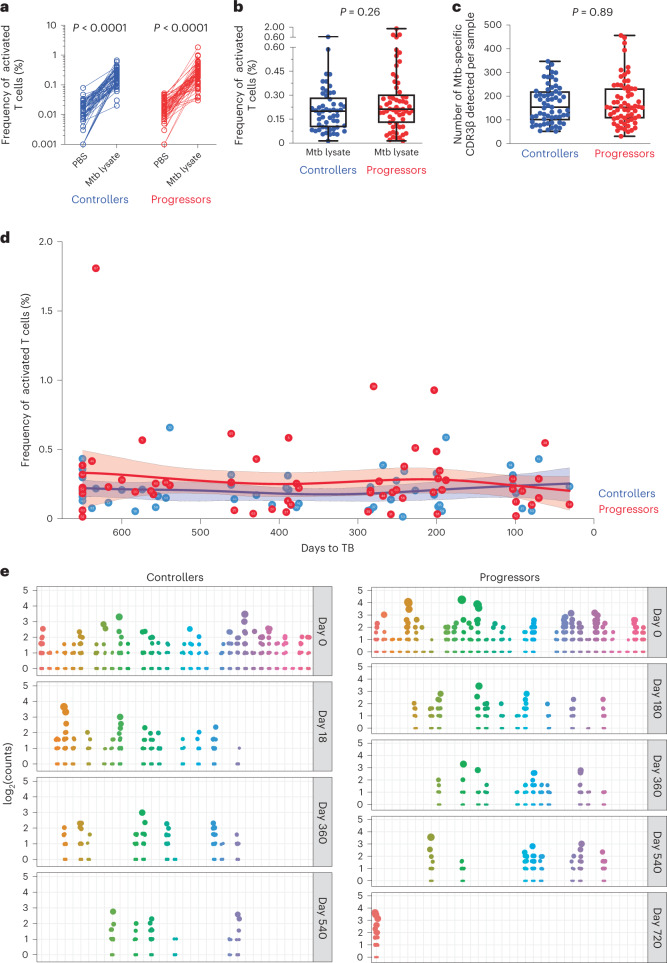
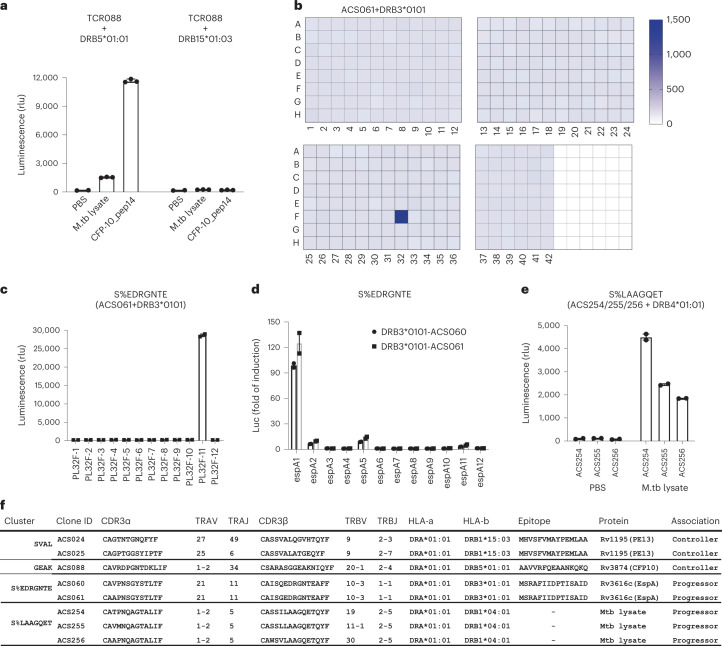
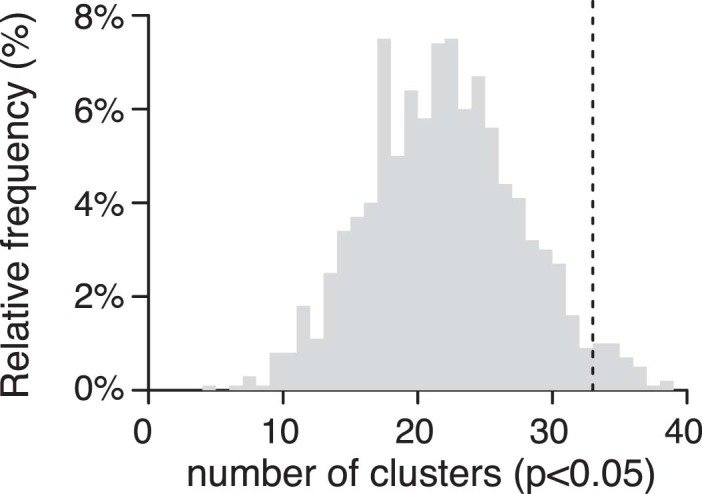
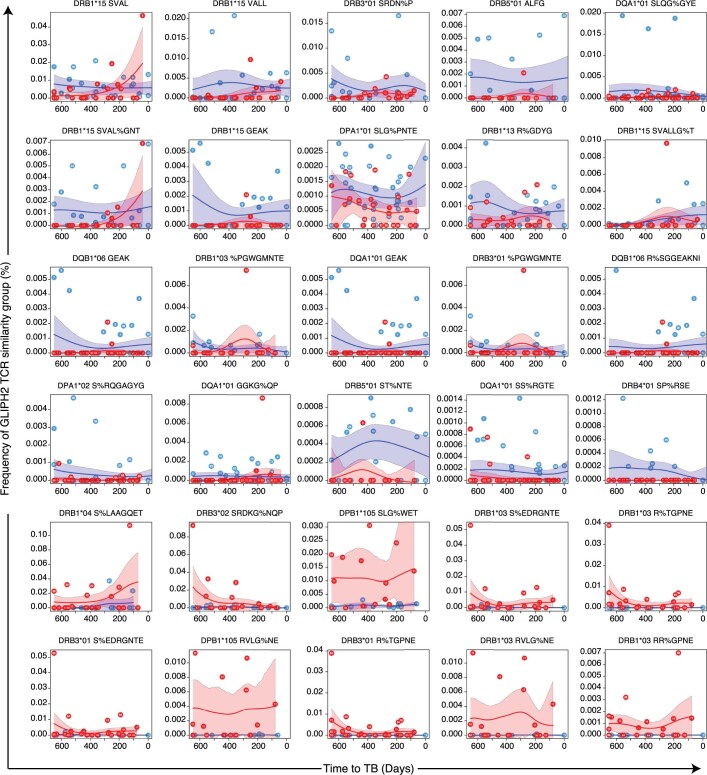
Antigen-specific, MHC-restricted αβ T cells are necessary for protective immunity against Mycobacterium tuberculosis, but the ability to broadly study these responses has been limited. In the present study, we used single-cell and bulk T cell receptor (TCR) sequencing and the GLIPH2 algorithm to analyze M. tuberculosis-specific sequences in two longitudinal cohorts, comprising 166 individuals with M. tuberculosis infection who progressed to either tuberculosis (n = 48) or controlled infection (n = 118). We found 24 T cell groups with similar TCR-β sequences, predicted by GLIPH2 to have common TCR specificities, which were associated with control of infection (n = 17), and others that were associated with progression to disease (n = 7). Using a genome-wide M. tuberculosis antigen screen, we identified peptides targeted by T cell similarity groups enriched either in controllers or in progressors. We propose that antigens recognized by T cell similarity groups associated with control of infection can be considered as high-priority targets for future vaccine development.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures











Comment in
-
Finding antigens for TB vaccines: the good, the bad and the useless.Nat Med. 2023 Jan;29(1):35-36. doi: 10.1038/s41591-022-02123-4. Nat Med. 2023. PMID: 36604539 Free PMC article.
-
Finding TB vaccine antigens: follow the TCRs.Sci Immunol. 2023 Feb 3;8(80):eadg8281. doi: 10.1126/sciimmunol.adg8281. Epub 2023 Feb 3. Sci Immunol. 2023. PMID: 36735772
References
-
- Scriba, T. J., Coussens, A. K. & Fletcher, H. A. Human immunology of tuberculosis. Microbiol. Spectr. 10.1128/microbiolspec.TBTB2-0016-2016 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
