

The effect of blood pressure on mortality following out-of-hospital cardiac arrest: a retrospective cohort study of the United Kingdom Intensive Care National Audit and Research Centre database
- PMID: 36604745
- PMCID: PMC9817239
- DOI: 10.1186/s13054-022-04289-2
The effect of blood pressure on mortality following out-of-hospital cardiac arrest: a retrospective cohort study of the United Kingdom Intensive Care National Audit and Research Centre database
Erratum in
-
Publisher Correction: The effect of blood pressure on mortality following out‑of‑hospital cardiac arrest: a retrospective cohort study of the United Kingdom Intensive Care National Audit and Research Centre database.Crit Care. 2023 May 4;27(1):169. doi: 10.1186/s13054-023-04458-x. Crit Care. 2023. PMID: 37143141 Free PMC article. No abstract available.
Abstract
Background: Hypotension following out-of-hospital cardiac arrest (OHCA) may cause secondary brain injury and increase mortality rates. Current guidelines recommend avoiding hypotension. However, the optimal blood pressure following OHCA is unknown. We hypothesised that exposure to hypotension and hypertension in the first 24 h in ICU would be associated with mortality following OHCA.
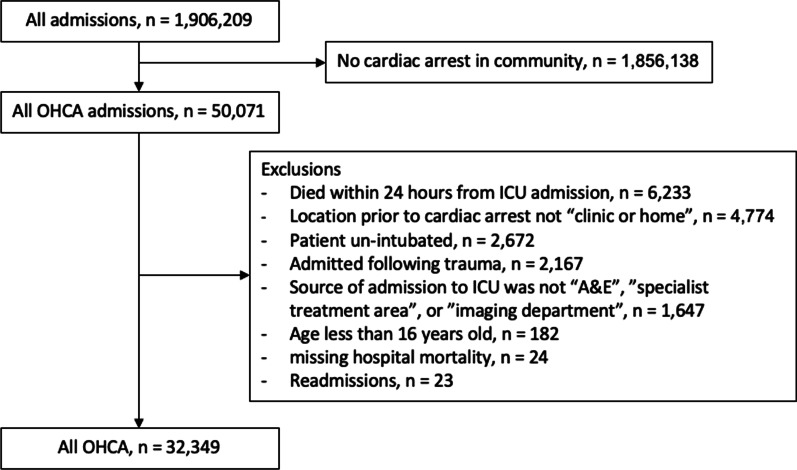
Methods: We conducted a retrospective analysis of OHCA patients included in the Intensive Care National Audit and Research Centre Case Mix Programme from 1 January 2010 to 31 December 2019. Restricted cubic splines were created following adjustment for important prognostic variables. We report the adjusted odds ratio for associations between lowest and highest mean arterial pressure (MAP) and systolic blood pressure (SBP) in the first 24 h of ICU care and hospital mortality.
Results: A total of 32,349 patients were included in the analysis. Hospital mortality was 56.2%. The median lowest and highest MAP and SBP were similar in survivors and non-survivors. Both hypotension and hypertension were associated with increased mortality. Patients who had a lowest recorded MAP in the range 60-63 mmHg had the lowest associated mortality. Patients who had a highest recorded MAP in the range 95-104 mmHg had the lowest associated mortality. The association between SBP and mortality followed a similar pattern to MAP.
Conclusions: We found an association between hypotension and hypertension in the first 24 h in ICU and mortality following OHCA. The inability to distinguish between the median blood pressure of survivors and non-survivors indicates the need for research into individualised blood pressure targets for survivors following OHCA.
Keywords: Blood pressure; Cardiac arrest; Critical care; Hypertension; Hypotension; Mean arterial pressure; Mortality; Systolic blood pressure.
© 2023. The Author(s).
Conflict of interest statement
Peter J. McGuigan declares that he has no conflict of interests. Elisa Giallongo declares that she has no conflict of interests. Prof Bronagh Blackwood declares that she has no conflict of interests. Dr James Doidge declares that he has no conflict of interests. Prof David A. Harrison declares that he has no conflict of interests. Prof Alistair D. Nichol declares that he has no conflict of interests. Prof Kathryn M. Rowan declares that she has no conflict of interests. Prof Manu Shankar-Hari declares that he has no conflict of interests. Prof Markus B. Skrifvars has received speakers fees from BARD Medical (Ireland). Karen Thomas declares that she has no conflict of interests. Danny F McAuley declares that he has no competing interests.
Figures

Comment in
-
Analysis of static parameters in retrospective studies: limitations and interpretation.Crit Care. 2023 Oct 23;27(1):404. doi: 10.1186/s13054-023-04691-4. Crit Care. 2023. PMID: 37872549 Free PMC article. No abstract available.
-
A reply to analysis of static parameters in retrospective studies: limitations and interpretation.Crit Care. 2023 Nov 2;27(1):423. doi: 10.1186/s13054-023-04709-x. Crit Care. 2023. PMID: 37919803 Free PMC article. No abstract available.
References
-
- Nolan JP, Orzechowska I, Harrison DA, Soar J, Perkins GD, Shankar-Hari M. Changes in temperature management and outcome after out-of-hospital cardiac arrest in United Kingdom intensive care units following publication of the targeted temperature management trial. Resuscitation. 2021;1(162):304–311. doi: 10.1016/j.resuscitation.2021.03.027. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
