

Scar conducting channel characterization to predict arrhythmogenicity during ventricular tachycardia ablation
- PMID: 36607130
- PMCID: PMC10062327
- DOI: 10.1093/europace/euac257
Scar conducting channel characterization to predict arrhythmogenicity during ventricular tachycardia ablation
Abstract
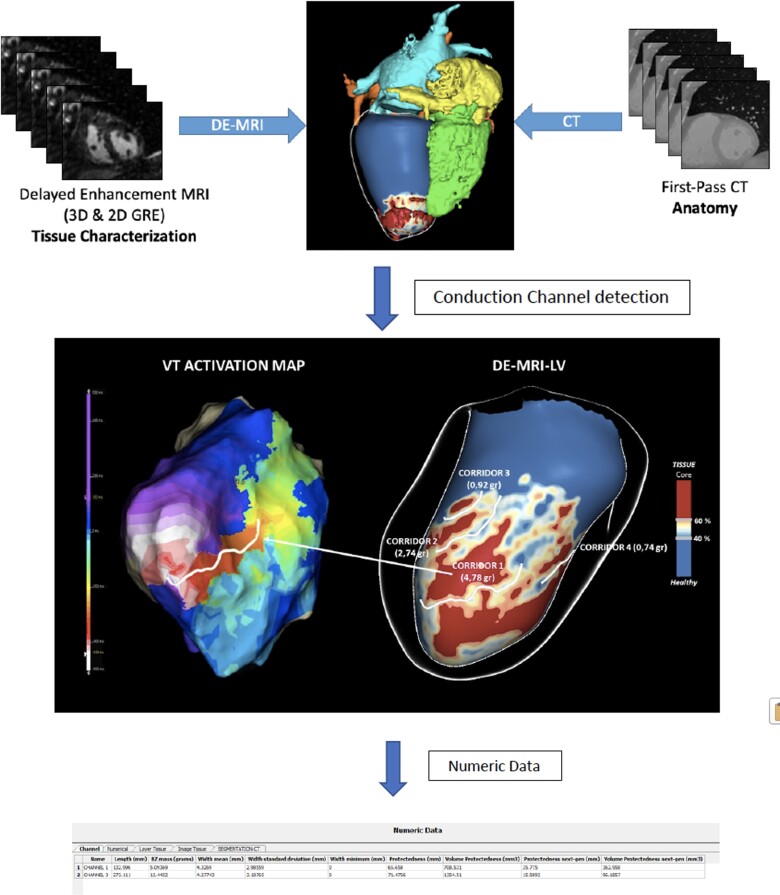
Aims: Heterogeneous tissue channels (HTCs) detected by late gadolinium enhancement cardiac magnetic resonance (LGE-CMR) are related to ventricular arrhythmias, but there are few published data about their arrhythmogenic characteristics.
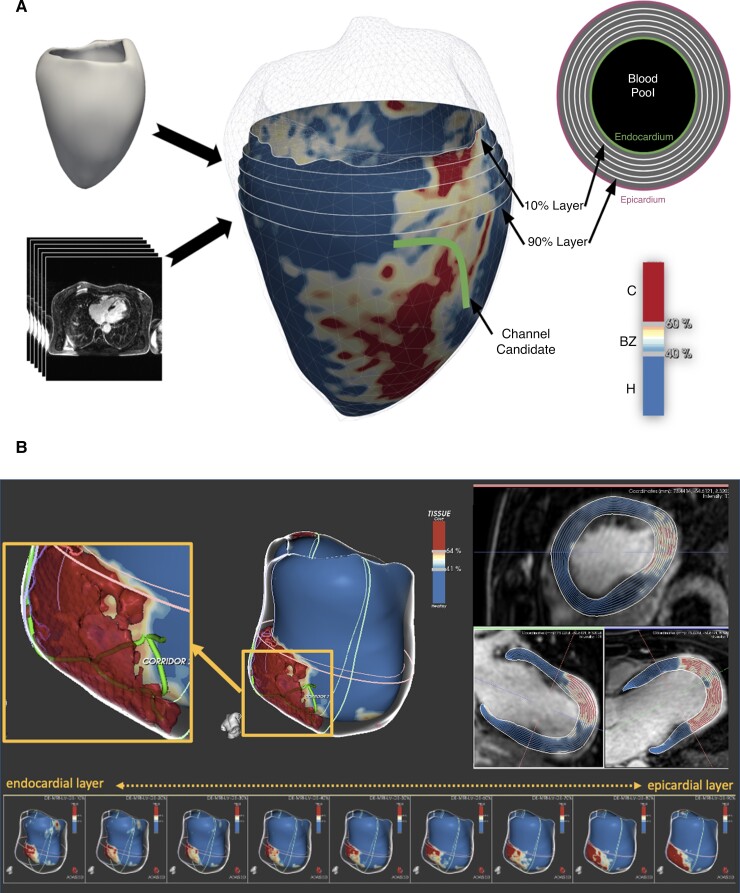
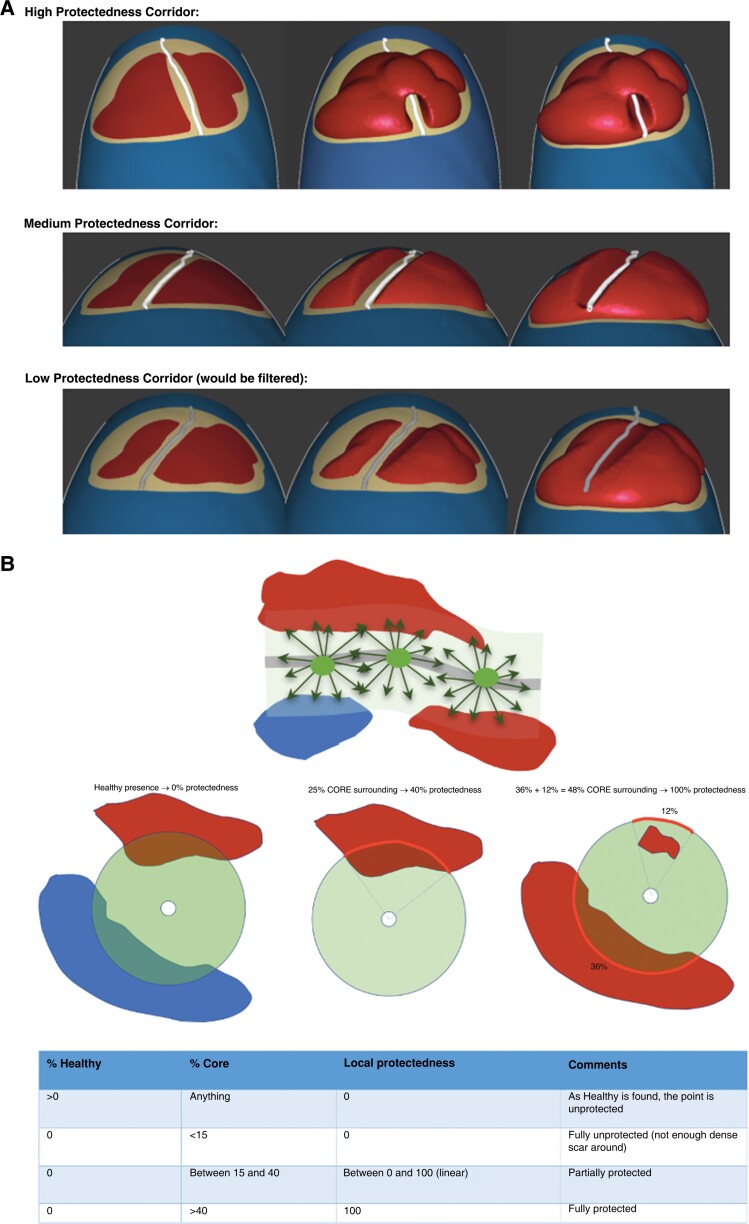
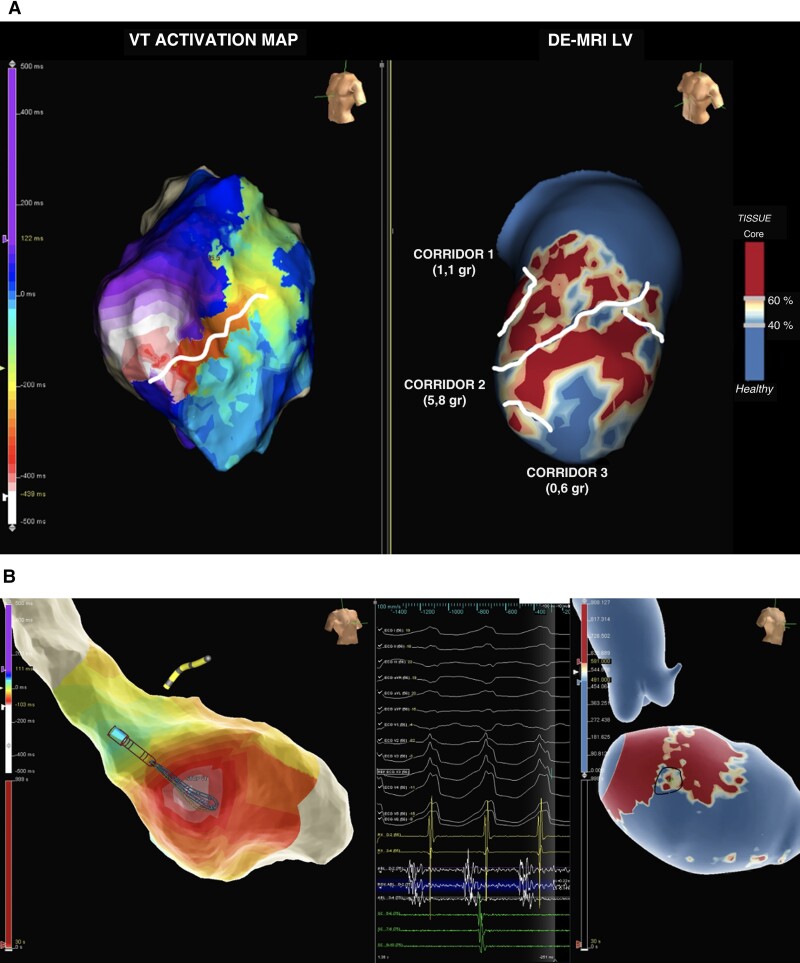
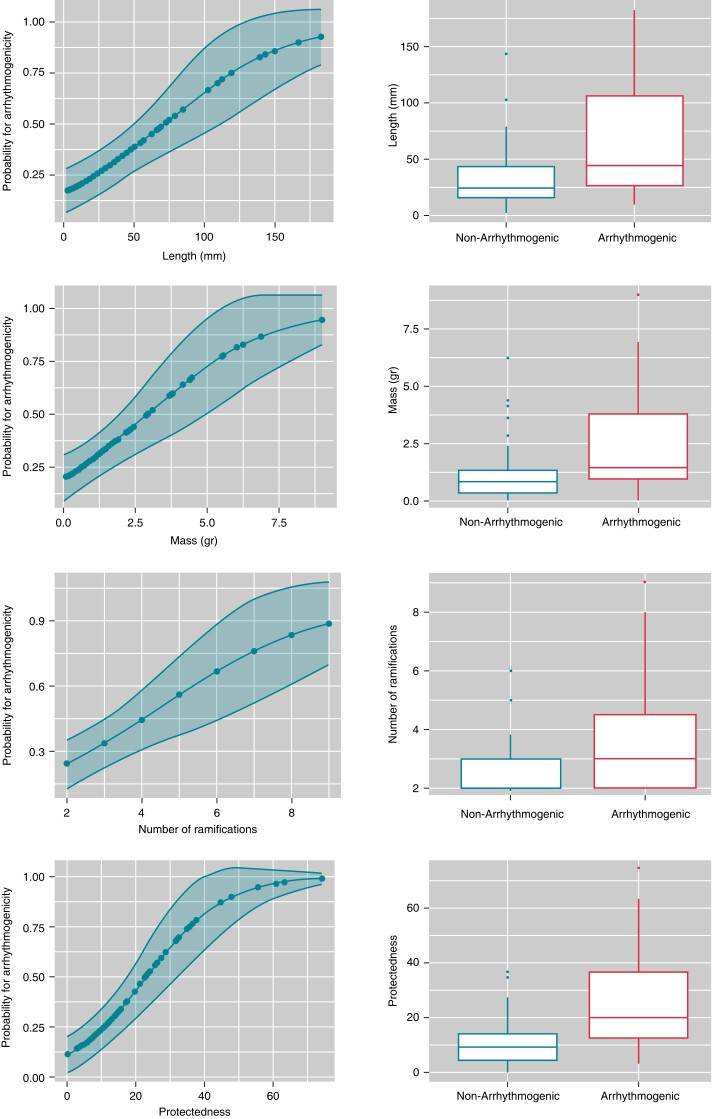
Methods and results: We enrolled 34 consecutive patients with ischaemic and non-ischaemic cardiomyopathy who were referred for ventricular tachycardia (VT) ablation. LGE-CMR was performed prior to ablation, and the HTCs were analyzed. Arrhythmogenic HTCs linked to induced VT were identified during the VT ablation procedure. The characteristics of arrhythmogenic HTCs were compared with those of non-arrhythmogenic HTCs. Three patients were excluded due to low-quality LGE-CMR images. A total of 87 HTCs were identified on LGE-CMR in 31 patients (age:63.8 ± 12.3 years; 96.8% male; left ventricular ejection fraction: 36.1 ± 10.7%). Of the 87 HTCs, only 31 were considered arrhythmogenic because of their relation to a VT isthmus. The HTCs related to a VT isthmus were longer [64.6 ± 49.4 vs. 32.9 ± 26.6 mm; OR: 1.02; 95% CI: (1.01-1.04); P < 0.001] and had greater mass [2.5 ± 2.2 vs. 1.2 ± 1.2 grams; OR: 1.62; 95% CI: (1.18-2.21); P < 0.001], a higher degree of protectedness [26.19 ± 19.2 vs. 10.74 ± 8.4; OR 1.09; 95% CI: (1.04-1.14); P < 0.001], higher transmurality [number of wall layers with CCs: 3.8 ± 2.4 vs. 2.4 ± 2.0; OR: 1.31; 95% CI: (1.07-1.60); P = 0.008] and more ramifications [3.8 ± 2.0 vs. 2.7 ± 1.1; OR: 1.59; 95% CI: (1.15-2.19); P = 0.002] than non-arrhythmogenic HTCs. Multivariate logistic regression analysis revealed that protectedness was the strongest predictor of arrhythmogenicity.
Conclusion: The protectedness of an HTC identified by LGE-CMR is strongly related to its arrhythmogenicity during VT ablation.
Keywords: Ventricular tachycardia; cardiac magnetic resonance; conducting channel; heterogeneous tissue channel; scar.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: I.R.L. and J.M.T. have served as consultants for Boston Scientific and Abbott Medical.L.M. and J.B. report activities as consultants, lecturers, and advisory board members for Abbott Medical, Boston Scientific, Biosense Webster, Medtronic, and Biotronik. They are also shareholders of Galgo Medical, S.L. M.S and R.FV work for ADAS3D Medical S.L. All other authors declare no conflict of interest.
Figures
References
-
- Wissner E, Stevenson WG, Kuck K-H. Catheter ablation of ventricular tachycardia in ischaemic and non-ischaemic cardiomyopathy: where are we today? A clinical review. Eur Heart J 2012;33:1440–50. - PubMed
-
- Stevenson WG, Khan H, Sager P, Saxon LA, Middlekauff HR, Natterson PDet al. Identification of reentry circuit sites during catheter mapping and radiofrequency ablation of ventricular tachycardia late after myocardial infarction. Circulation 1993;88(4):1647–70. - PubMed
-
- Fitzgerald DM, Friday KJ, Wah JA, Lazzara R, Jackman WM. Electrogram patterns predicting successful catheter ablation of ventricular tachycardia. Circulation 1988;77(4):806–14. - PubMed
-
- Andreu D, Berruezo A, Ortiz-Pérez JT, Silva E, Mont L, Borràs Ret al. Integration of 3D electroanatomic maps and magnetic resonance scar characterization into the navigation system to guide ventricular tachycardia ablation. Circulation: Arrhythmia and Electrophysiology 2011;4(5):674–83. - PubMed
-
- Quinto L, Sanchez-Somonte P, Alarcón F, Garre P, Castillo À, San Antonio Ret al. Ventricular tachycardia burden reduction after substrate ablation: predictors of recurrence. Heart Rhythm 2021;18(6):896–904. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
