

Benefits of secretion clearance with high frequency percussive ventilation in tracheostomized critically ill patients: a pilot study
- PMID: 36607533
- PMCID: PMC10175357
- DOI: 10.1007/s10877-022-00970-7
Benefits of secretion clearance with high frequency percussive ventilation in tracheostomized critically ill patients: a pilot study
Abstract
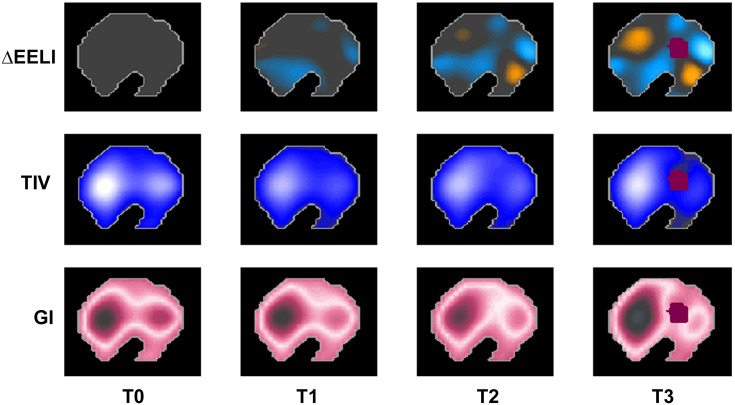
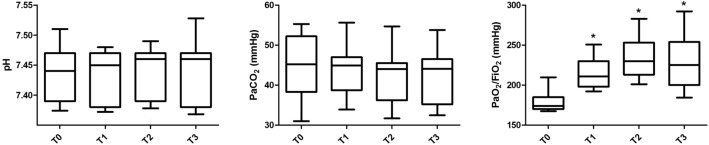
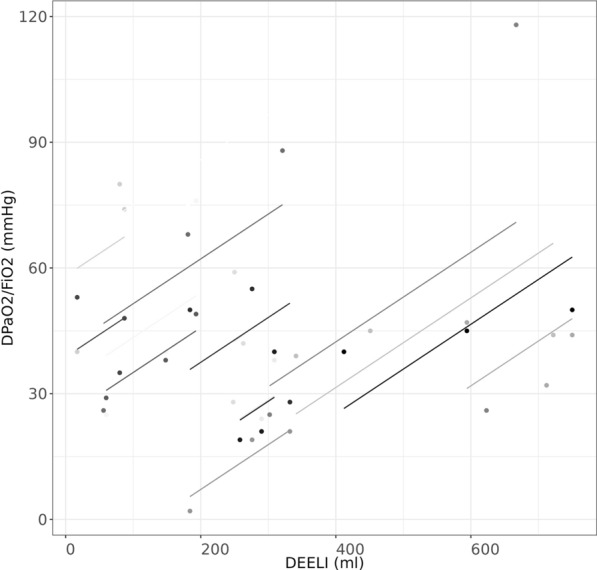
Clearance of secretions remains a challenge in ventilated patients. Despite high-frequency percussive ventilation (HFPV) showing benefits in patients with cystic fibrosis and neuromuscular disorders, very little is known about its effects on other patient categories. Therefore, we designed a physiological pilot study investigating the effects on lung aeration and gas exchange of short HFPV cycles in tracheostomized patients undergoing mechanical ventilation. Electrical impedance tomography (EIT) was recorded at baseline (T0) by a belt wrapped around the patient's chest, followed by the HFPV cycle lasting 10 min. EIT data was collected again after the HFPV cycle (T1) as well as after 1 h (T2) and 3 h (T3) from T0. Variation from baseline of end-expiratory lung impedance (∆EELI), tidal variation (TIV) and global inhomogeneity index (GI) were computed. Arterial blood was also taken for gas analysis. HFPV cycle significantly improved the ∆EELI at T1, T2 and T3 when compared to baseline (p < 0.05 for all comparisons). The ratio between arterial partial pressure and inspired fraction of oxygen (PaO2/FiO2) also increased after the treatment (p < 0.001 for all comparison) whereas TIV (p = 0.132) and GI (p = 0.114) remained unchanged. Short cycles of HFPV superimposed to mechanical ventilation promoted alveolar recruitment, as suggested by improved ∆EELI, and improved oxygenation in tracheostomized patients with high load of secretion.Trial Registration Prospectively registered on www.clinicaltrials.gov (NCT05200507; dated 6th January 2022).
Keywords: Acute respiratory failure; Chest physiotherapy; Cough; Electrical impedance tomography; High-frequency percussive ventilation; Lung aeration.
© 2023. The Author(s).
Conflict of interest statement
Prof. Longhini received honoraria/speaking fees from Fisher & Paykel, Draeger and Intersurgical. Prof. Navalesi’s research laboratory has received equipment and grants from Draeger and Intersurgical S.p.A. He also received honoraria/speaking fees from Philips, ResMed, MSD and Novartis. Prof. Navalesi contributed to the development of the helmet Next, whose licence for patent belongs to Intersurgical S.P.A. and receives royalties for that invention. Prof. Longhini and Prof. Navalesi contributed to the development of a new device not discussed in the present study (European Patent number 3320941 released on 5th August 2020) and they are designated as inventors. The remaining authors have no conflict of interest to disclose.
Figures
References
-
- Pneumatikos IA, Dragoumanis CK, Bouros DE. Ventilator-associated pneumonia or endotracheal tube-associated pneumonia? An approach to the pathogenesis and preventive strategies emphasizing the importance of endotracheal tube. Anesthesiology. 2009;110(3):673–680. doi: 10.1097/ALN.0b013e31819868e0. - DOI - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
