

Laparoscopic fundoplication performed in community hospital settings: A protocol for systematic review
- PMID: 36607888
- PMCID: PMC9829280
- DOI: 10.1097/MD.0000000000032502
Laparoscopic fundoplication performed in community hospital settings: A protocol for systematic review
Abstract
Background: Laparoscopic fundoplication (LF) is well-established as the surgical intervention of choice for management of refactory gastro-esophageal reflux disease. Much of its success lies in the reported benefits in symptom control outlined by the postoperative patient. It is unclear whether patient-reported outcomes differ according to the institution type providing care. This review aimed to address this knowledge gap by reviewing the available evidence examining patient-reported outcomes of LF in non-metropolitan centers.
Objectives: To investigate patient-reported outcomes of LF performed in regional or community-based hospitals.
Data sources: Four electronic databases, and citations of relevant articles.
Study eligibility criteria: Only studies that separately reported patient-reported outcomes of LF performed in regional or community hospitals were included; papers deemed to be unclear about the type of facility in which LF surgeries were performed, or in which data from LF surgeries performed in regional/community hospitals was combined with data from major metropolitan hospitals, were excluded.
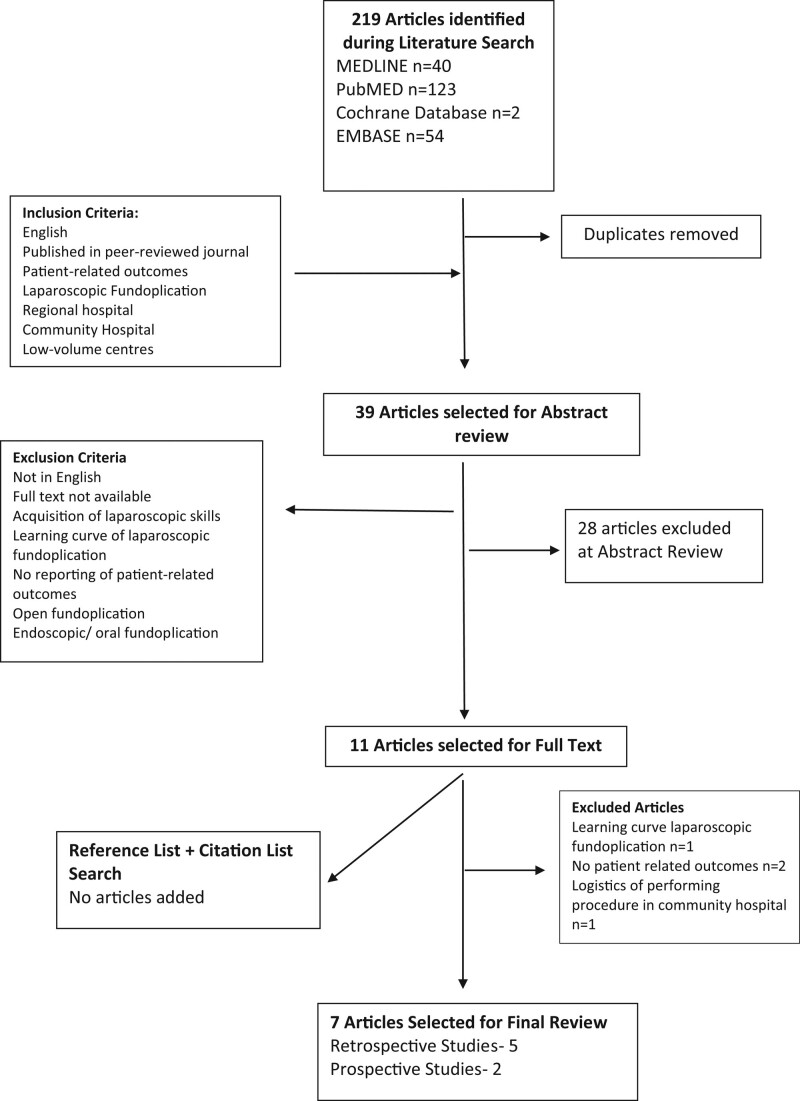
Study appraisal: Only studies that were graded as fair or good using Quality Assessment Tool for Observational Cohort and Cross-sectional studies were eligible for inclusion in this review. Seven studies were then eligible for inclusion, all of which were observational cohort studies with 6 of the studies reporting on a single intervention arm.
Results: Seven observational cohort studies were included in the review, with a combined total of 1071 patients who underwent LF at non-metropolitan centers. Of these, data was collected for 742 patients, yielding an overall response rate of 69.3%. All 7 studies assessed patients' post-operative outcomes through questionnaires that were based on a modified Likert scale or a similar tool. Overall patient satisfaction was high (86%) and a significant majority of patients stated they would recommend the procedure to others (93.3%). Post-operative prevalence of reflux and dysphagia compared favorably to rates generally reported in the literature (11.9% and 17.6% respectively). Further research is required to ascertain the safety of performing these procedures in non-metropolitan hospitals.
Conclusion: Current evidence suggests that patient-reported outcomes are favorable for patients undergoing LF in community settings, and are broadly comparable to those undergoing LF in tertiary-level centers.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
References
-
- Vakil N, van Zanten SV, Kahrilas P, et al. . The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Consensus development conference research support, non-U.S. Gov’t systematic review. Am J Gastroenterol. 2006;101:1900–20. quiz 1943. - PubMed
-
- Fuchs KH, Babic B, Breithaupt W, et al. . EAES recommendations for the management of gastroesophageal reflux disease. Consensus development conference practice guideline research support, non-U.S. Gov’t. Surg Endosc. 2014;28:1753–73. - PubMed
-
- Fock KM, Talley N, Goh KL, et al. . Asia-Pacific consensus on the management of gastro-oesophageal reflux disease: an update focusing on refractory reflux disease and Barrett’s oesophagus. Gut. 2016;65:1402–15. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
