

Ibrutinib for First-Line Treatment of Chronic Graft-Versus-Host Disease: Results From the Randomized Phase III iNTEGRATE Study
- PMID: 36608310
- PMCID: PMC10082299
- DOI: 10.1200/JCO.22.00509
Ibrutinib for First-Line Treatment of Chronic Graft-Versus-Host Disease: Results From the Randomized Phase III iNTEGRATE Study
Abstract
Purpose: To present primary and final analyses from the randomized, double-blind, placebo-controlled, phase III iNTEGRATE study, which evaluated the safety and efficacy of ibrutinib with prednisone in previously untreated patients with chronic graft-versus-host disease (cGVHD).
Methods: Patients (age ≥ 12 years) with newly diagnosed moderate or severe cGVHD, requiring systemic corticosteroid therapy, and with no prior systemic treatment for cGVHD were randomly assigned 1:1 to receive ibrutinib 420 mg once daily plus prednisone, starting at 1 mg/kg once daily or placebo plus prednisone. The primary end point was response rate at 48 weeks according to 2014 National Institutes of Health Consensus Development Project Criteria. Other end points included event-free survival, duration of response, time to withdrawal of immunosuppressants, improvement in Lee cGVHD Symptom Scale score, overall survival (OS), and safety.
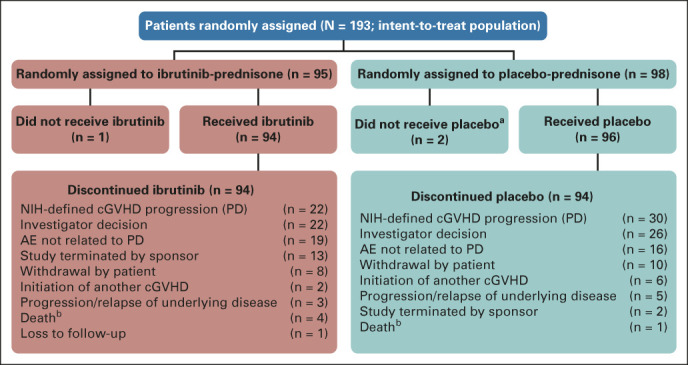
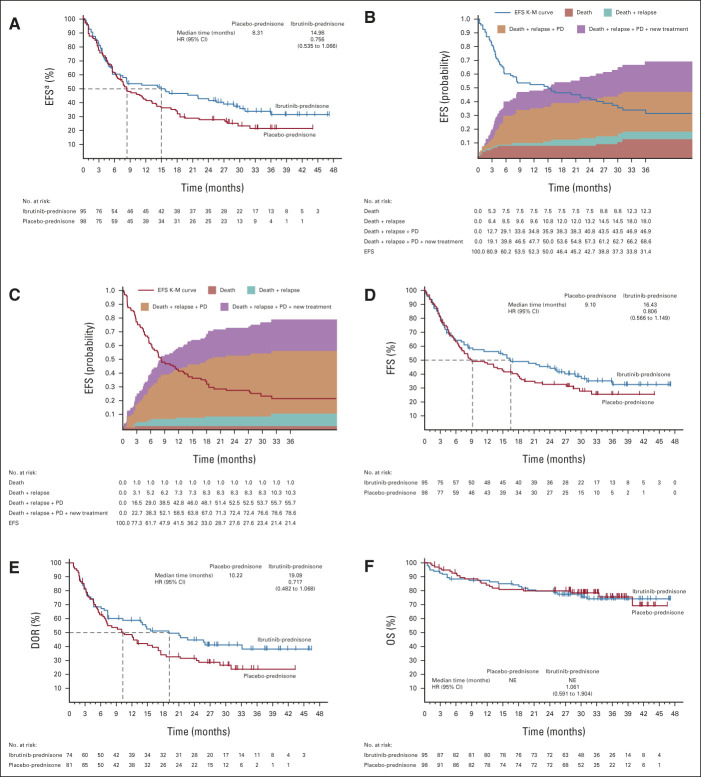
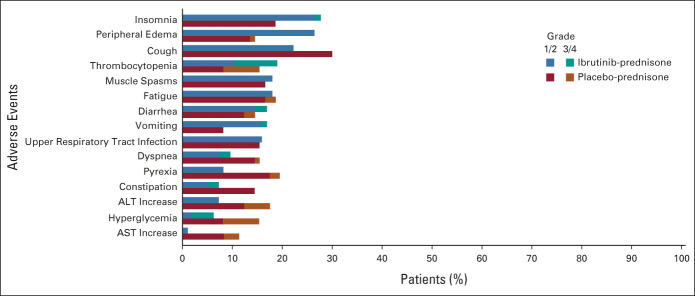
Results: Ninety-five and 98 patients enrolled in the ibrutinib-prednisone and placebo-prednisone arms, respectively. At 48 weeks, response rates were 41% (ibrutinib-prednisone) and 37% (placebo-prednisone; P = .54). At 33 months of follow-up, median duration of response was 19 months (ibrutinib-prednisone) and 10 months (placebo-prednisone; P = .10). Median event-free survival was 15 months (ibrutinib-prednisone) and 8 months (placebo-prednisone; hazard ratio, 0.76; 95% CI, 0.54 to 1.1; P = .11). Improvement in overall Lee cGVHD Symptom Scale was 43% (ibrutinib-prednisone) and 31% (placebo-ibrutinib; P = .07). Median OS was not reached in either arm. The 24-month Kaplan-Meier OS estimates were 80% for both arms (hazard ratio, 1.06; 95% CI, 0.59 to 1.90). Grade ≥ 3 serious adverse events occurred in 49% (ibrutinib-prednisone) and 47% (placebo-prednisone) of patients.
Conclusion: There was no statistical difference observed in the primary and secondary end points with ibrutinib-prednisone treatment. No new safety signals were observed with ibrutinib treatment in previously untreated patients with cGVHD. The primary end point of iNTEGRATE was not met.
Trial registration: ClinicalTrials.gov NCT02959944.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
References
-
- Lee SJ, Klein JP, Barrett AJ, et al. : Severity of chronic graft-versus-host disease: Association with treatment-related mortality and relapse. Blood 100:406-414, 2002 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
