

Cost-effectiveness and budget impact of adding tranexamic acid for management of post-partum hemorrhage in the Indian public health system
- PMID: 36609241
- PMCID: PMC9817327
- DOI: 10.1186/s12884-022-05308-4
Cost-effectiveness and budget impact of adding tranexamic acid for management of post-partum hemorrhage in the Indian public health system
Abstract
Background: Postpartum hemorrhage (PPH) is the global leading cause of maternal mortality, affecting nearly 3 to 6 percent of all women giving birth in India. The World Health Organization (WHO) has updated its guidelines to recommend the early use of intravenous (IV) tranexamic acid (TXA) in addition to standard care for all diagnosed PPH cases. This study aimed to assess the cost-effectiveness of introducing TXA for PPH management in the Indian public health system.
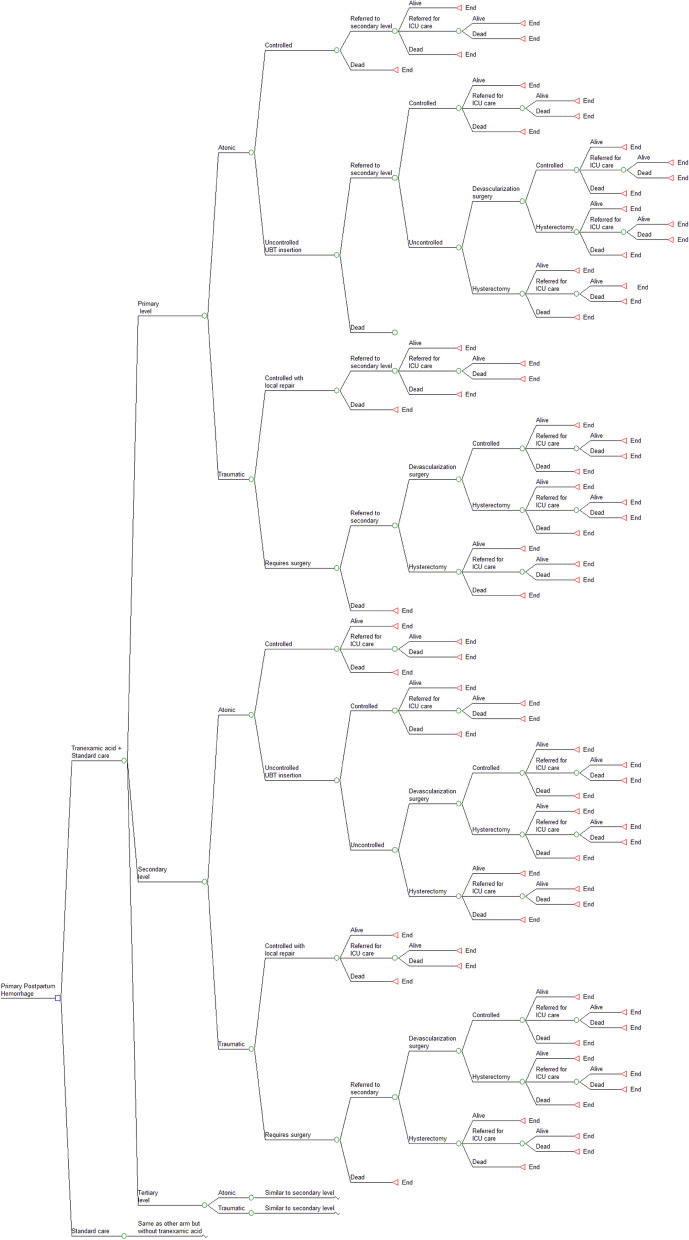
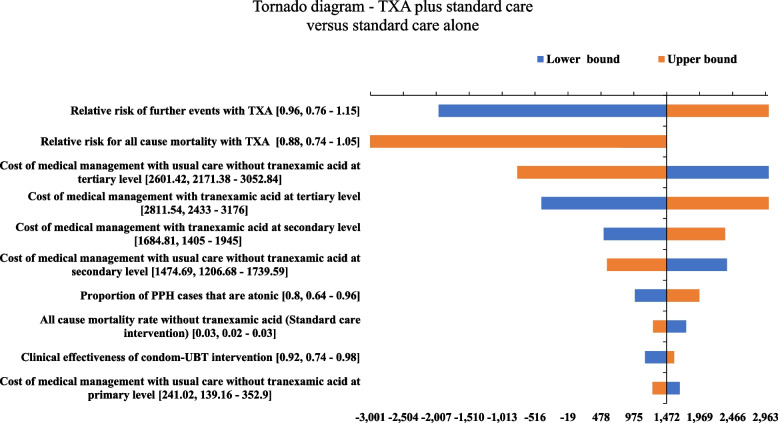
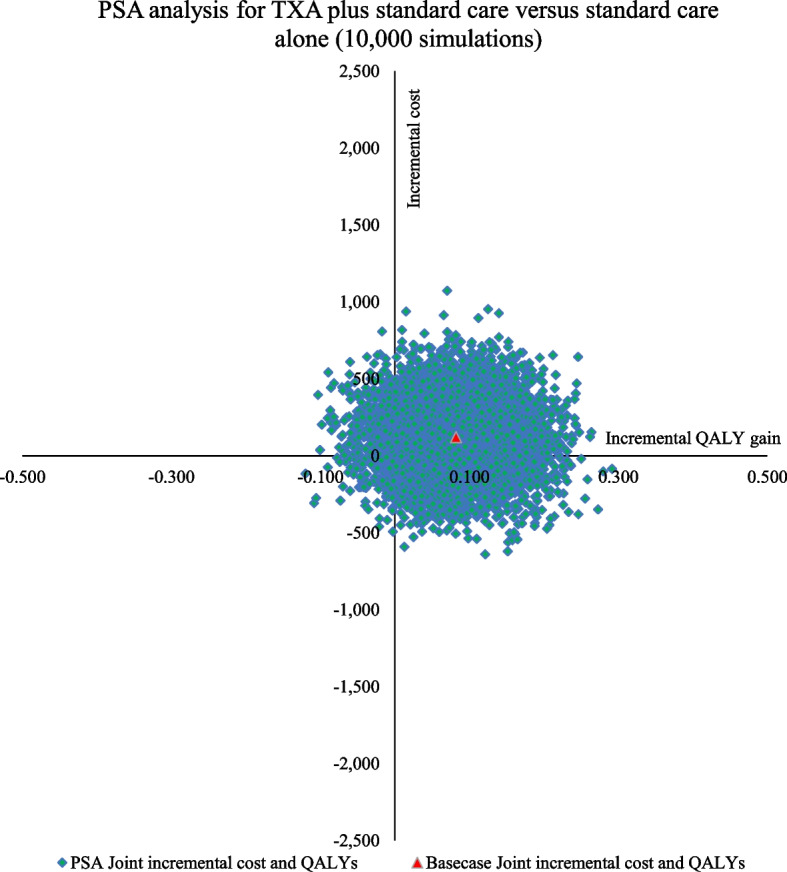
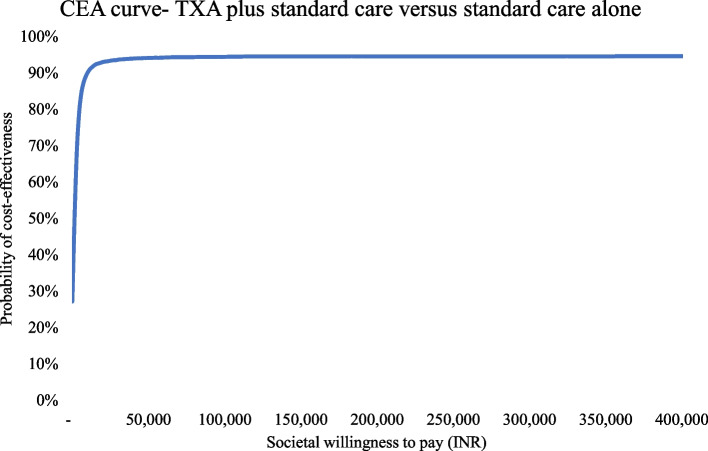
Methods: A decision analytic model was built using a decision tree to determine the cost-effectiveness of administering IV TXA to women experiencing PPH within 3 h of birth to existing management with uterotonics and supportive care. Using a disaggregated societal perspective, the costs and consequences for a hypothetical cohort of women experiencing PPH in public health facilities was estimated. The model was populated using probabilities, clinical parameters, and utilities from published literature, while cost parameters were largely derived from a primary economic costing study. The primary outcome of interest was the incremental cost-utility ratio (ICUR). Associated clinical events and net benefits were estimated. One-way and probabilistic sensitivity analysis (PSA) was undertaken. The budget impact was estimated for a national-level introduction.
Results: For an estimated annual cohort of 510,915 PPH cases in India, the addition of IV TXA would result in a per-patient disaggregated societal cost of INR 6607 (USD 95.15) with a discounted gain of 20.25 QALYs, as compared to a cost of INR 6486 (USD 93.41) with a discounted gain of 20.17 QALYs with standard care PPH management. At an ICUR value of INR 1470 per QALY gained (USD 21), the addition of IV TXA is cost-effective in Indian public health settings. The intervention is likely to prevent 389 maternal deaths, 177 surgeries, and 128 ICU admissions per 100,000 PPH cases. The findings are robust under uncertainty, with 94.5% of PSA simulations remaining cost-effective. A cumulative increase of 2.3% financial allocation for PPH management over five years will be incurred for TXA introduction.
Conclusions: Addition of tranexamic acid for primary PPH management, as recommended by WHO, is cost-effective in Indian public health settings. Policy guidelines, training manuals, and facility checklists should be updated to reflect this recommendation.
Keywords: Cost-effectiveness; IV TXA; Maternal mortality; Postpartum hemorrhage; Primary PPH management; Tranexamic acid.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Cost-effectiveness of uterine balloon tamponade devices in managing atonic post-partum hemorrhage at public health facilities in India.PLoS One. 2021 Aug 18;16(8):e0256271. doi: 10.1371/journal.pone.0256271. eCollection 2021. PLoS One. 2021. PMID: 34407132 Free PMC article.
-
Tranexamic acid in the routine treatment of postpartum hemorrhage in the United States: a cost-effectiveness analysis.Am J Obstet Gynecol. 2019 Sep;221(3):275.e1-275.e12. doi: 10.1016/j.ajog.2019.06.030. Epub 2019 Jun 18. Am J Obstet Gynecol. 2019. PMID: 31226298
-
Tranexamic acid for treatment of women with post-partum haemorrhage in Nigeria and Pakistan: a cost-effectiveness analysis of data from the WOMAN trial.Lancet Glob Health. 2018 Feb;6(2):e222-e228. doi: 10.1016/S2214-109X(17)30467-9. Lancet Glob Health. 2018. PMID: 29389542 Free PMC article. Clinical Trial.
-
Tranexamic Acid for Postpartum Hemorrhage Treatment in Low-Resource Settings: A Rapid Scoping Review.Int J Environ Res Public Health. 2022 Jun 16;19(12):7385. doi: 10.3390/ijerph19127385. Int J Environ Res Public Health. 2022. PMID: 35742634 Free PMC article.
-
Cost Effectiveness of Introducing Etonorgestrel Contraceptive Implant into India's Current Family Welfare Programme.Appl Health Econ Health Policy. 2021 Mar;19(2):267-277. doi: 10.1007/s40258-020-00605-5. Appl Health Econ Health Policy. 2021. PMID: 32776166
Cited by
-
The cost-effectiveness of preventing, diagnosing, and treating postpartum haemorrhage: A systematic review of economic evaluations.PLoS Med. 2024 Sep 13;21(9):e1004461. doi: 10.1371/journal.pmed.1004461. eCollection 2024 Sep. PLoS Med. 2024. PMID: 39269991 Free PMC article.
References
-
- Goal 3 | Department of Economic and Social Affairs. https://sdgs.un.org/goals/goal3. Accessed 12 Jan 2022.
-
- World Health Organization. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. 2019.
-
- Maternal Mortality. https://www.gatesfoundation.org/goalkeepers/report/2021-report/progress-.... Accessed 12 Mar 2022.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
