

An exosome-based liquid biopsy signature for pre-operative identification of lymph node metastasis in patients with pathological high-risk T1 colorectal cancer
- PMID: 36609320
- PMCID: PMC9817247
- DOI: 10.1186/s12943-022-01685-8
An exosome-based liquid biopsy signature for pre-operative identification of lymph node metastasis in patients with pathological high-risk T1 colorectal cancer
Abstract
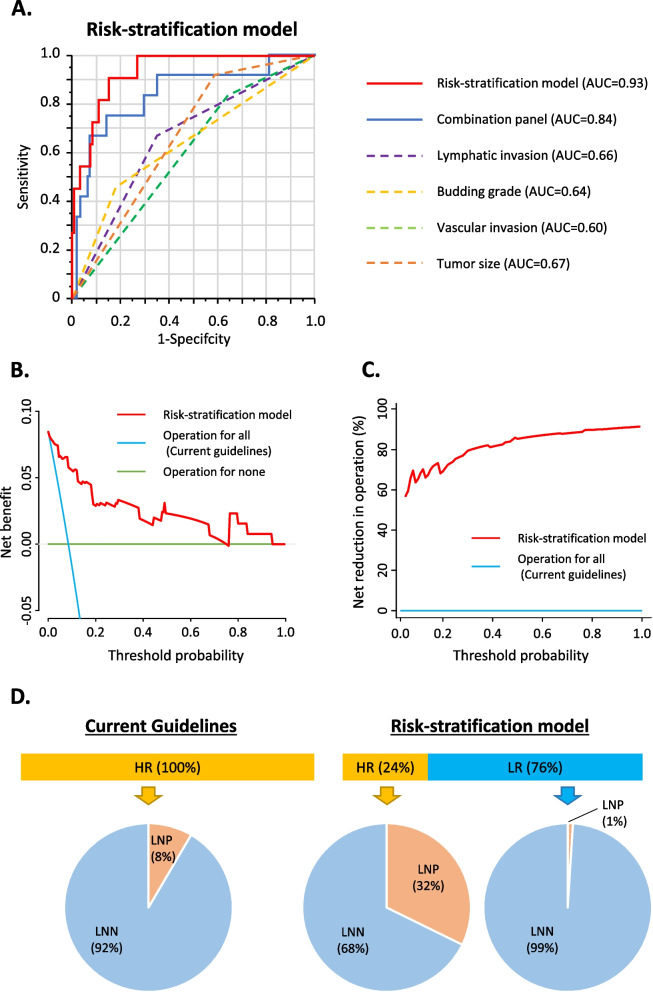
Background: According to current guidelines, more than 70% of patients with invasive submucosal colorectal cancer (T1 CRC) undergo a radical operation with lymph node dissection, even though only ~ 10% have lymph node metastasis (LNM). Hence, there is imperative to develop biomarkers that can help robustly identify LNM-positive patients to prevent such overtreatments. Given the emerging interest in exosomal cargo as a source for biomarker development in cancer, we examined the potential of exosomal miRNAs as LNM prediction biomarkers in T1 CRC.
Methods: We analyzed 200 patients with high-risk T1 CRC from two independent cohorts, including a training (n = 58) and a validation cohort (n = 142). Cell-free and exosomal RNAs from pre-operative serum were extracted, followed by quantitative reverse-transcription polymerase chain reactions for a panel of miRNAs.
Results: A panel of four miRNAs (miR-181b, miR-193b, miR-195, and miR-411) exhibited robust ability for detecting LNM in the exosomal vs. cell-free component. We subsequently established a cell-free and exosomal combination signature, successfully validated in two independent clinical cohorts (AUC, 0.84; 95% CI 0.70-0.98). Finally, we developed a risk-stratification model by including key pathological features, which reduced the false positive rates for LNM by 76% without missing any true LNM-positive patients.
Conclusions: Our novel exosomal miRNA-based liquid biopsy signature robustly identifies T1 CRC patients at risk of LNM in a preoperative setting. This could be clinically transformative in reducing the significant overtreatment burden of this malignancy.
Keywords: Cell-free miRNA; Exosomal miRNA; Liquid biopsy; Lymph node metastasis; T1 CRC.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
