

Reduced time to imaging, length of stay, and hospital charges following implementation of a novel postoperative pathway for craniotomy
- PMID: 36609368
- PMCID: PMC10904334
- DOI: 10.3171/2022.12.JNS222123
Reduced time to imaging, length of stay, and hospital charges following implementation of a novel postoperative pathway for craniotomy
Abstract
Objective: The authors created a postoperative postanesthesia care unit (PACU) pathway to bypass routine intensive care unit (ICU) admissions of patients undergoing routine craniotomies, to improve ICU resource utilization and reduce overall hospital costs and lengths of stay while maintaining quality of care and patient satisfaction. In the present study, the authors evaluated this novel PACU-to-floor clinical pathway for a subset of patients undergoing craniotomy with a case time under 5 hours and blood loss under 500 ml.
Methods: A single-institution retrospective cohort study was performed to compare 202 patients enrolled in the PACU-to-floor pathway and 193 historical controls who would have met pathway inclusion criteria. The pathway cohort consisted of all adult supratentorial brain tumor cases from the second half of January 2021 to the end of January 2022 that met the study inclusion criteria. Control cases were selected from the beginning of January 2020 to halfway through January 2021. The authors also discuss common themes of similar previously published pathways and the logistical and clinical barriers overcome for successful PACU pathway implementation.
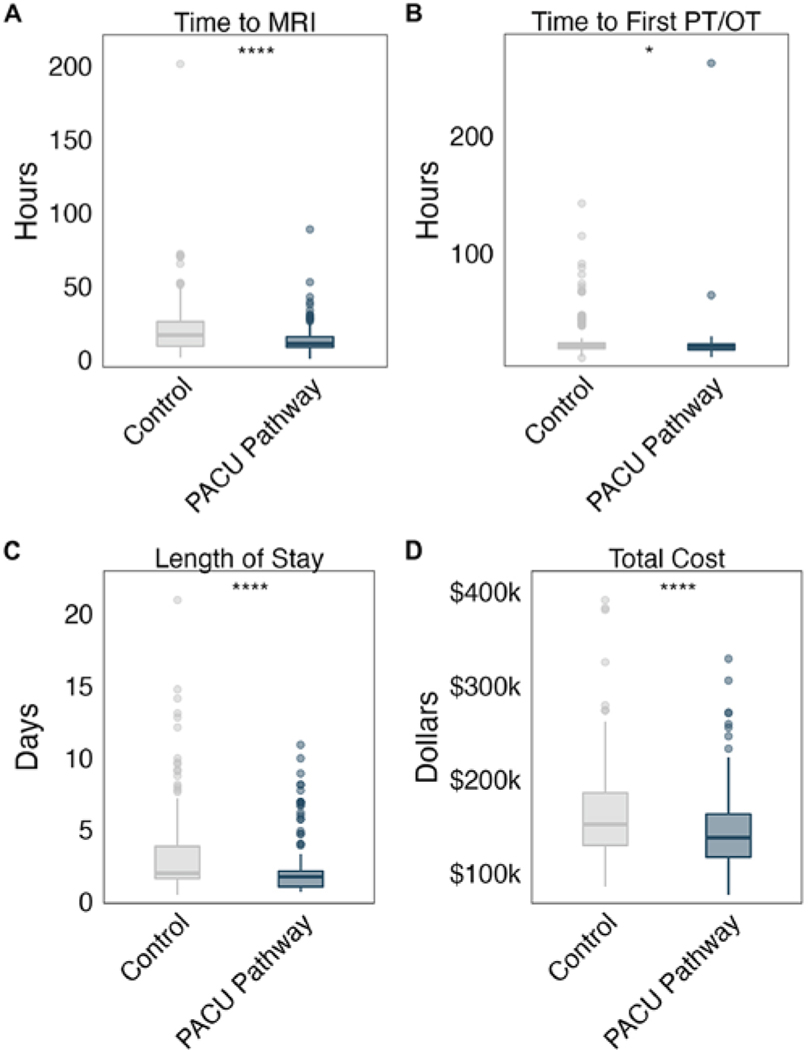
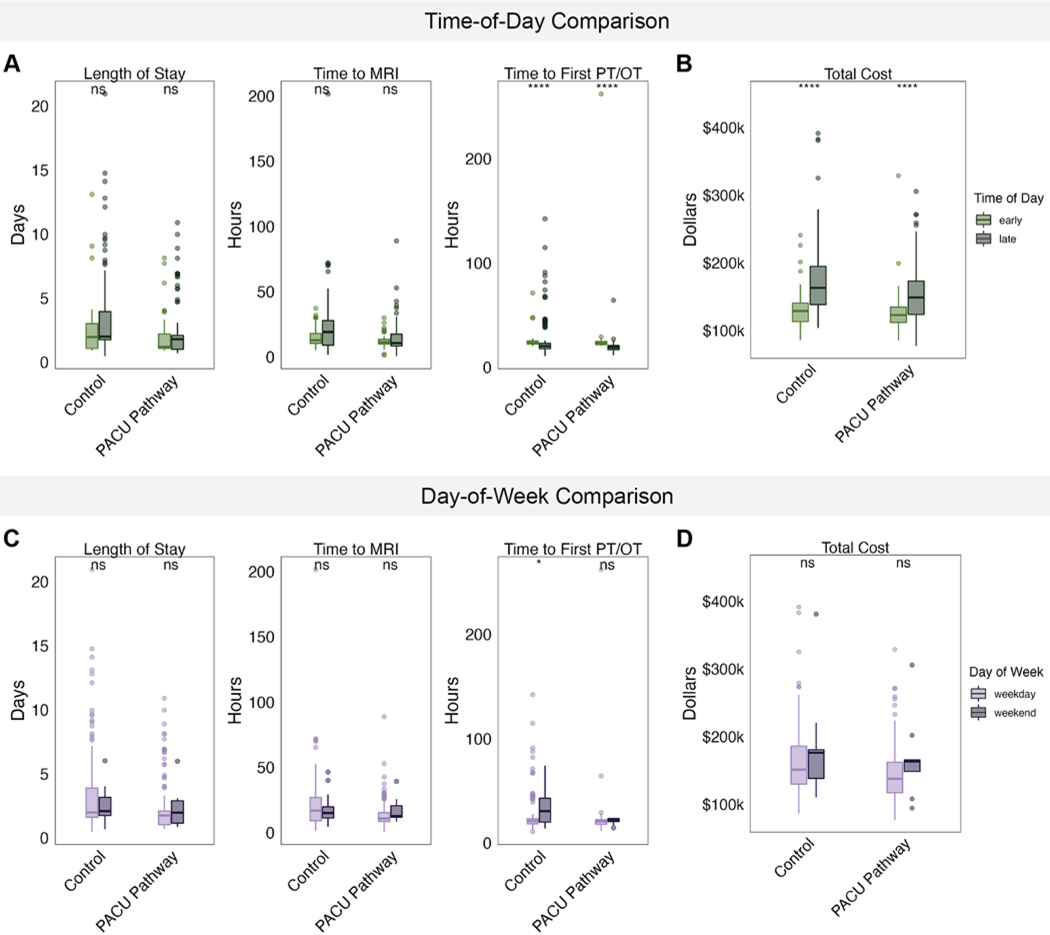
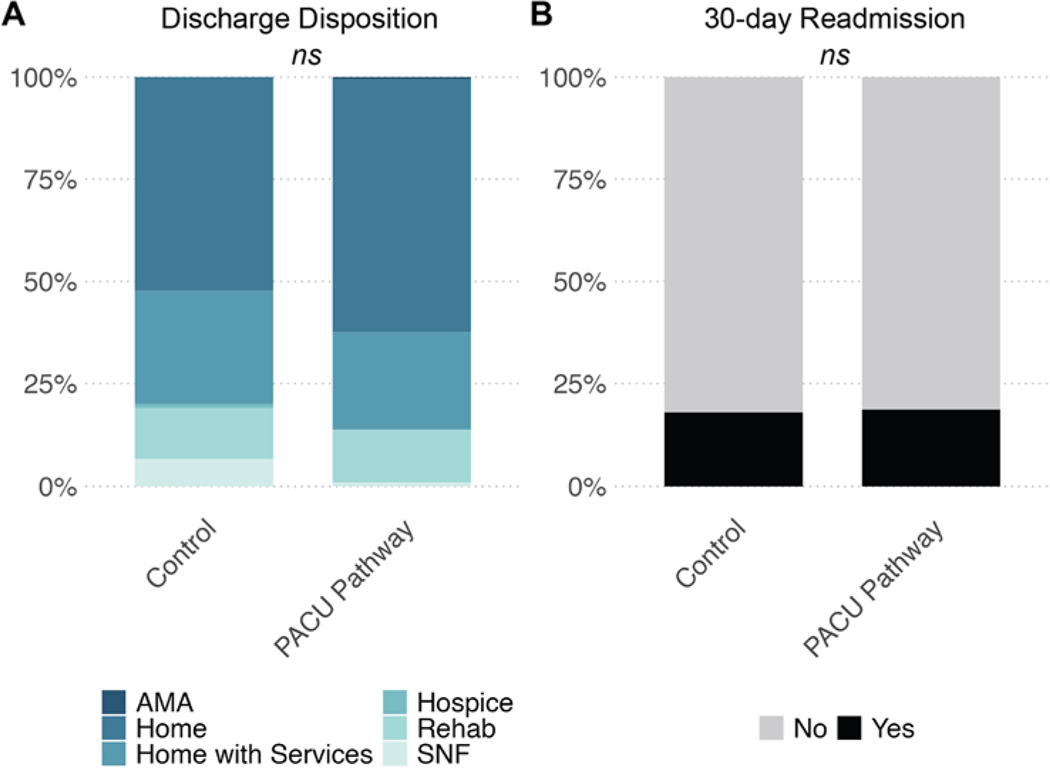
Results: Pathway enrollees had a median age of 61 years (IQR 49-69 years) and 53% were female. Age, sex, pathology, and American Society of Anesthesiologists physical status distributions were similar between pathway and control patients (p > 0.05). Most of the pathway cases (96%) were performed on weekdays, and 31% had start times before noon. Nineteen percent of pathway patients had 30-day readmissions, most frequently for headache (16%) and syncope (10%), whereas 18% of control patients had 30-day readmissions (p = 0.897). The average time to MRI was 6 hours faster for pathway patients (p < 0.001) and the time to inpatient physical therapy and/or occupational therapy evaluation was 4.1 hours faster (p = 0.046). The average total length of stay was 0.7 days shorter for pathway patients (p = 0.02). A home discharge occurred in 86% of pathway cases compared to 81% of controls (p = 0.225). The average total hospitalization charges were $13,448 lower for pathway patients, representing a 7.4% decrease (p = 0.0012, adjusted model). Seven pathway cases were escalated to the ICU postoperatively because of attending physician preference (2 cases), agitation (1 case), and new postoperative neurological deficits (4 cases), resulting in a 96.5% rate of successful discharge from the pathway. In bypassing the ICU, critical care resource utilization was improved by releasing 0.95 ICU days per patient, or 185 ICU days across the cohort.
Conclusions: The featured PACU-to-floor pathway reduces the stay of postoperative craniotomy patients and does not increase the risk of early hospital readmission.
Keywords: craniotomy; neurosurgery outcomes; postoperative pathway; tumor.
Figures
Similar articles
-
A Safe Transitions Pathway for post-craniotomy neurological surgery patients: high-value care that bypasses the intensive care unit.J Neurosurg. 2020 May 29;134(5):1386-1391. doi: 10.3171/2020.3.JNS192133. Print 2021 May 1. J Neurosurg. 2020. PMID: 32470928
-
Cost-effectiveness development for the postoperative care of craniotomy patients: a safe transitions pathway in neurological surgery.Neurosurg Focus. 2018 May;44(5):E19. doi: 10.3171/2018.2.FOCUS1812. Neurosurg Focus. 2018. PMID: 29712529
-
Routine use of postoperative ICU care for elective craniotomy: a cost-benefit analysis.Surg Neurol. 2003 Dec;60(6):483-9; dicussion 489. doi: 10.1016/s0090-3019(03)00517-2. Surg Neurol. 2003. PMID: 14670660
-
Reexamining the Role of Postoperative ICU Admission for Patients Undergoing Elective Craniotomy: A Systematic Review.Crit Care Med. 2022 Sep 1;50(9):1380-1393. doi: 10.1097/CCM.0000000000005588. Epub 2022 Jun 10. Crit Care Med. 2022. PMID: 35686911
-
The Utility of Routine Intensive Care Admission for Patients Undergoing Intracranial Neurosurgical Procedures: A Systematic Review.Neurocrit Care. 2018 Feb;28(1):35-42. doi: 10.1007/s12028-017-0433-4. Neurocrit Care. 2018. PMID: 28808901
Cited by
-
Mobilization in Neurocritical Care: Challenges and Opportunities.Curr Neurol Neurosci Rep. 2024 Dec 26;25(1):13. doi: 10.1007/s11910-024-01399-y. Curr Neurol Neurosci Rep. 2024. PMID: 39722066 Free PMC article. Review.
-
Postoperative Surveillance in the Postoperative vs. Intensive Care Unit for Patients Undergoing Elective Supratentorial Brain Tumor Removal: A Retrospective Observational Study.J Clin Med. 2025 Apr 11;14(8):2632. doi: 10.3390/jcm14082632. J Clin Med. 2025. PMID: 40283463 Free PMC article.
-
Routine ICU Surveillance after Brain Tumor Surgery: Patient Selection Using Machine Learning.J Clin Med. 2024 Sep 26;13(19):5747. doi: 10.3390/jcm13195747. J Clin Med. 2024. PMID: 39407807 Free PMC article.
-
Postoperative Monitoring After Elective Intracranial Surgery in a Postanesthesia Care Unit is Safe, Efficient, and Cost-Effective.Neurocrit Care. 2025 Jul 21. doi: 10.1007/s12028-025-02323-z. Online ahead of print. Neurocrit Care. 2025. PMID: 40691410
References
-
- Nitahara JA, Valencia M, Bronstein MA. Medical case management after laminectomy or craniotomy: do all patients benefit from admission to the intensive care unit? Neurosurg Focus. 1998; 5(2): e4. - PubMed
-
- de Almeida CC, Boone MD, Laviv Y, Kasper BS, Chen CC, Kasper EM. The utility of routine intensive care admission for patients undergoing intracranial neurosurgical procedures: a systematic review. Neurocrit Care. 2018; 28(1): 35–42. - PubMed
-
- Beauregard CL, Friedman WA. Routine use of postoperative ICU care for elective craniotomy: a cost-benefit analysis. Surg Neurol. 2003; 60(6): 483–489. - PubMed
-
- Florman JE, Cushing D, Keller LA, Rughani AI. A protocol for postoperative admission of elective craniotomy patients to a non-ICU or step-down setting. J Neurosurg. 2017; 127(6): 1392–1397. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
