

Treatment escalation patterns to start biologics in refractory moderate juvenile dermatomyositis among members of the Childhood Arthritis and Rheumatology Research Alliance
- PMID: 36609397
- PMCID: PMC9825021
- DOI: 10.1186/s12969-022-00785-5
Treatment escalation patterns to start biologics in refractory moderate juvenile dermatomyositis among members of the Childhood Arthritis and Rheumatology Research Alliance
Abstract
Background: Despite new and better treatments for juvenile dermatomyositis (JDM), not all patients with moderate severity disease respond adequately to first-line therapy. Those with refractory disease remain at higher risk for disease and glucocorticoid-related complications. Biologic disease-modifying antirheumatic drugs (DMARDs) have become part of the arsenal of treatments for JDM. However, prospective comparative studies of commonly used biologics are lacking.
Methods: The Childhood Arthritis and Rheumatology Research Alliance (CARRA) JDM biologics workgroup met in 2019 and produced a survey assessing current treatment escalation practices for JDM, including preferences regarding use of biologic treatments. The cases and questions were developed using a consensus framework, requiring 80% agreement for consensus. The survey was completed online in 2020 by CARRA members interested in JDM. Survey results were analyzed among all respondents and according to years of experience. Chi-square or Fisher's exact test was used to compare the distribution of responses to each survey question.
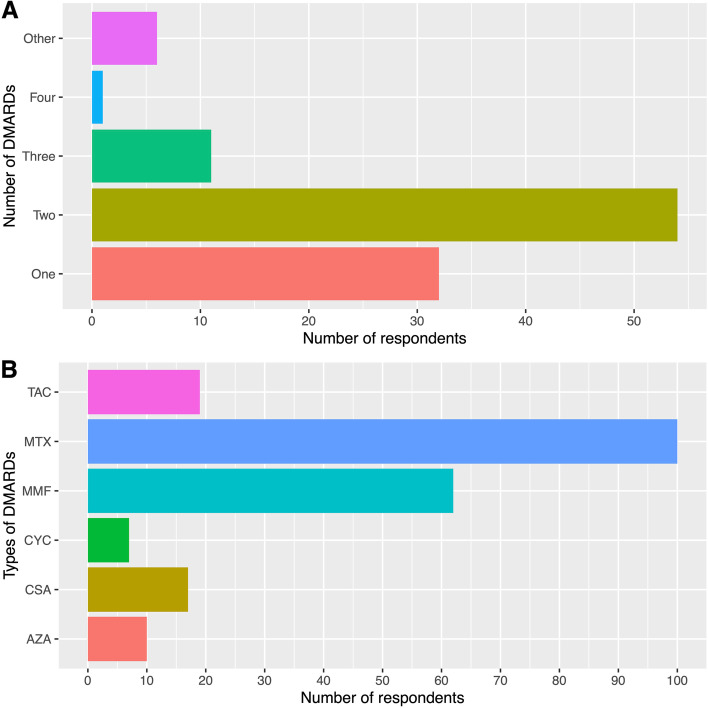
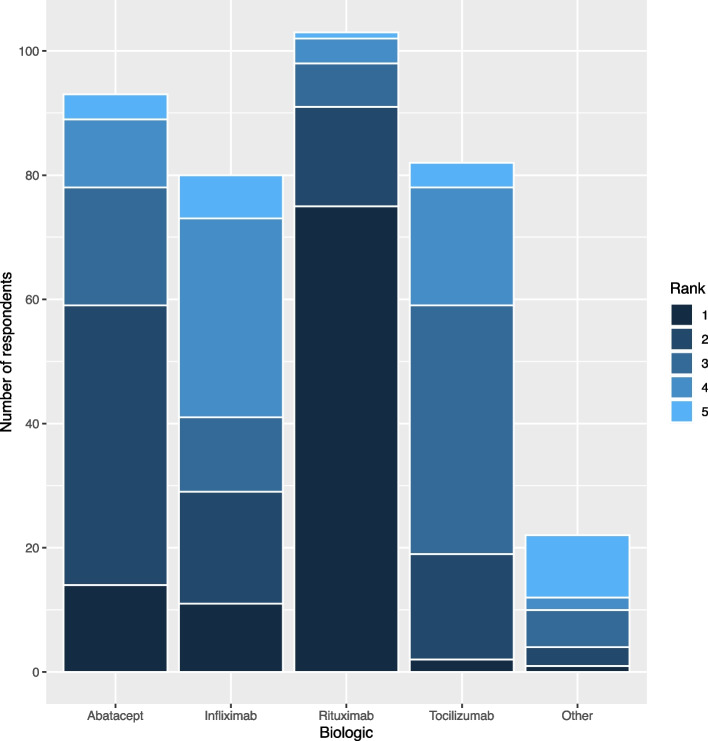
Results: One hundred twenty-one CARRA members responded to the survey (denominators vary for each question). Of the respondents, 88% were pediatric rheumatologists, 85% practiced in the United States, and 43% had over 10 years of experience. For a patient with moderately severe JDM refractory to methotrexate, glucocorticoids, and IVIG, approximately 80% of respondents indicated that they would initiate a biologic after failing 1-2 non-biologic DMARDs. Trials of methotrexate and mycophenolate were considered necessary by 96% and 60% of respondents, respectively, before initiating a biologic. By weighed average, rituximab was the preferred biologic over abatacept, tocilizumab, and infliximab. Over 50% of respondents would start a biologic by 4 months from diagnosis for patients with refractory moderately severe JDM. There were no notable differences in treatment practices between respondents by years of experience.
Conclusion: Most respondents favored starting a biologic earlier in disease course after trialing up to two conventional DMARDs, specifically including methotrexate. There was a clear preference for rituximab. However, there remains a dearth of prospective data comparing biologics in refractory JDM. These findings underscore the need for biologic consensus treatment plans (CTPs) for refractory JDM, which will ultimately facilitate comparative effectiveness studies and inform treatment practices.
Keywords: Biologics; Dmards; Juvenile dermatomyositis.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
CHS is co-Editor-in-Chief of Pediatric Rheumatology. The other authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
