

Use of serial smartphone-based assessments to characterize diverse neuropsychiatric symptom trajectories in a large trauma survivor cohort
- PMID: 36609484
- PMCID: PMC9823011
- DOI: 10.1038/s41398-022-02289-y
Use of serial smartphone-based assessments to characterize diverse neuropsychiatric symptom trajectories in a large trauma survivor cohort
Abstract
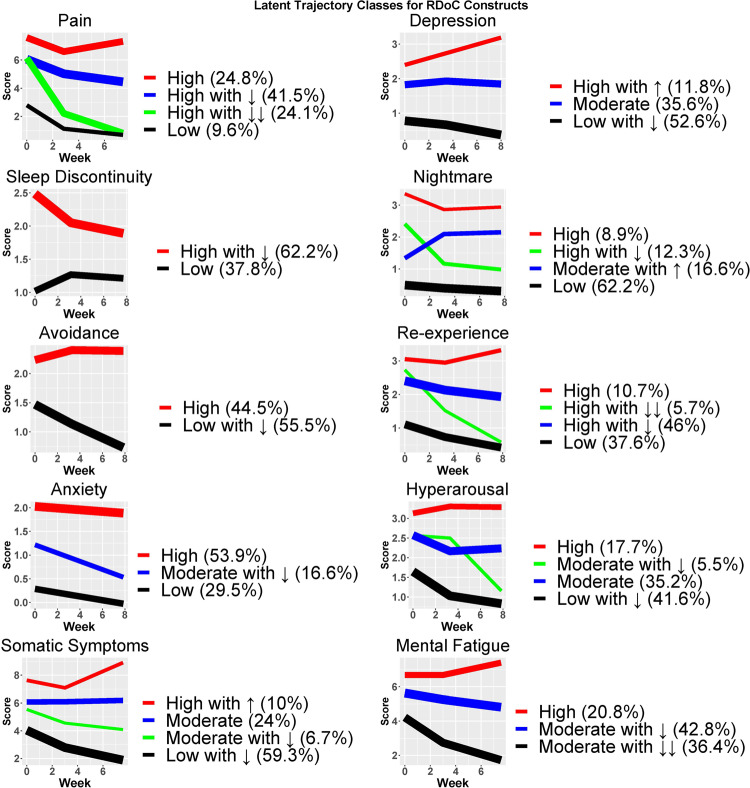
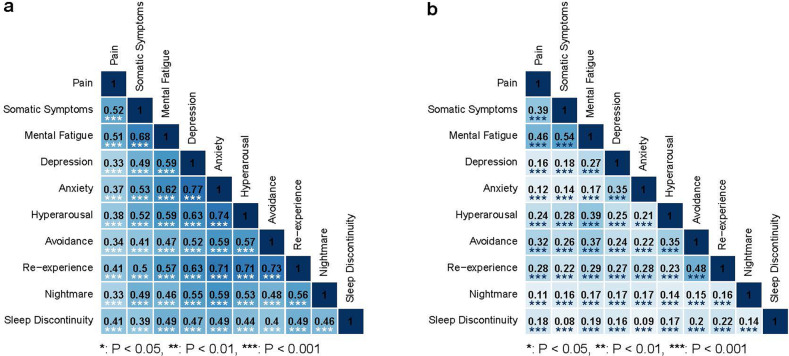
The authors sought to characterize adverse posttraumatic neuropsychiatric sequelae (APNS) symptom trajectories across ten symptom domains (pain, depression, sleep, nightmares, avoidance, re-experiencing, anxiety, hyperarousal, somatic, and mental/fatigue symptoms) in a large, diverse, understudied sample of motor vehicle collision (MVC) survivors. More than two thousand MVC survivors were enrolled in the emergency department (ED) and completed a rotating battery of brief smartphone-based surveys over a 2-month period. Measurement models developed from survey item responses were used in latent growth curve/mixture modeling to characterize homogeneous symptom trajectories. Associations between individual trajectories and pre-trauma and peritraumatic characteristics and traditional outcomes were compared, along with associations within and between trajectories. APNS across all ten symptom domains were common in the first two months after trauma. Many risk factors and associations with high symptom burden trajectories were shared across domains. Both across and within traditional diagnostic boundaries, APNS trajectory intercepts, and slopes were substantially correlated. Across all domains, symptom severity in the immediate aftermath of trauma (trajectory intercepts) had the greatest influence on the outcome. An interactive data visualization tool was developed to allow readers to explore relationships of interest between individual characteristics, symptom trajectories, and traditional outcomes ( http://itr.med.unc.edu/aurora/parcoord/ ). Individuals presenting to the ED after MVC commonly experience a broad constellation of adverse posttraumatic symptoms. Many risk factors for diverse APNS are shared. Individuals diagnosed with a single traditional outcome should be screened for others. The utility of multidimensional categorizations that characterize individuals across traditional diagnostic domains should be explored.
© 2023. The Author(s).
Conflict of interest statement
In the past 3 years, Dr. Kessler was a consultant for Datastat, Inc., RallyPoint Networks, Inc., Sage Pharmaceuticals, and Takeda. In the last three years, Dr. Clifford has received research funding from the NSF, NIH, and LifeBell AI, and unrestricted donations from AliveCor, Amazon Research, the Center for Discovery, the Gordon and Betty Moore Foundation, MathWorks, Microsoft Research, the Gates Foundation, Google, One Mind Foundation, and Samsung Research. Dr. Clifford has a financial interest in AliveCor and receives unrestricted funding from the company. He also is the CTO of MindChild Medical and CSO of LifeBell AI and has ownership in both companies. These relationships are unconnected to the current work. Dr. Germine is on the scientific advisory board of the nonprofit Sage Bionetworks, for which she receives a small honorarium. Dr. Sheikh has received funding from the Florida Medical Malpractice Joint Underwriter’s Association Dr. Alvin E. Smith Safety of Healthcare Services Grant, Allergan Foundation, the NIH/NIA-funded Jacksonville Aging Studies Center (JAX-ASCENT; R33AG05654), the Substance Abuse and Mental Health Services Administration (1H79TI083101-01), and the Florida Blue Foundation. Dr. Jones reports no direct conflicts related to this paper and no ongoing conflicts. He has been an investigator on studies funded by Hologic Inc., Janssen, and AstraZeneca, for which his department has received research funding. Over the past 3 years, Dr. Pizzagalli has received consulting fees from BlackThorn Therapeutics, Boehringer Ingelheim, Compass Pathway, Concert Pharmaceuticals, Engrail Therapeutics, Neurocrine Biosciences, Otsuka Pharmaceuticals, and Takeda Pharmaceuticals; one honorarium from Alkermes, and research funding from Millennium Pharmaceuticals. In addition, he has received stock options from BlackThorn Therapeutics. No funding from these entities was used to support the current work, and all views expressed are solely those of the authors. Dr. Elliott reports support from the National Institutes of Health (NIH) through Grant Numbers R01HD079076 & R03HD094577, Eunice Kennedy Shriver National Institute of Child Health & Human Development, National Center for Medical Rehabilitation Research, and consulting fees (<$15,000 per annum) from Orofacial Therapeutics, LLC. Dr. Ressler has served on advisory boards for Takeda, Resilience Therapeutics, Janssen, and Verily/Google. His research has been sponsored by Alkermes and Brainsway and he has worked as a consultant for Alkermes. Dr. McLean served as a consultant for Walter Reed and for Arbor Medical Innovations. The remaining authors declare no competing interests.
Figures
References
-
- National Center for Health Statistics. NHAMCS micro-data file. Hyattsville, MD, 2016.
-
- Beaudoin FL, Gutman R, Merchant RC, Clark MA, Swor RA, Jones JS, et al. Persistent pain after motor vehicle collision: comparative effectiveness of opioids vs nonsteroidal antiinflammatory drugs prescribed from the emergency department—a propensity matched analysis. Pain. 2017;158:289–95.. doi: 10.1097/j.pain.0000000000000756. - DOI - PMC - PubMed
