

Hemolytic disease of the fetus and newborn: systematic literature review of the antenatal landscape
- PMID: 36611144
- PMCID: PMC9824959
- DOI: 10.1186/s12884-022-05329-z
Hemolytic disease of the fetus and newborn: systematic literature review of the antenatal landscape
Abstract
Background: Prevention of pregnancy-related alloimmunization and the management of hemolytic disease of the fetus and newborn (HDFN) has significantly improved over the past decades. Considering improvements in HDFN care, the objectives of this systematic literature review were to assess the prenatal treatment landscape and outcomes of Rh(D)- and K-mediated HDFN in mothers and fetuses, to identify the burden of disease, to identify evidence gaps in the literature, and to provide recommendations for future research.
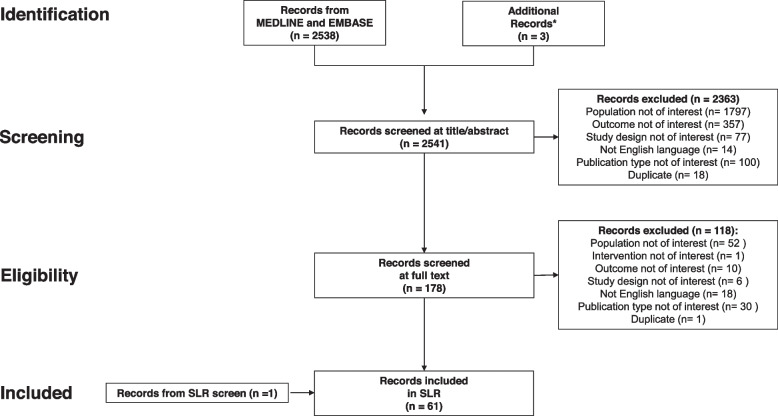
Methods: We performed a systematic search on MEDLINE, EMBASE and clinicaltrials.gov. Observational studies, trials, modelling studies, systematic reviews of cohort studies, and case reports and series of women and/or their fetus with HDFN caused by Rhesus (Rh)D or Kell alloimmunization. Extracted data included prevalence; treatment patterns; clinical outcomes; treatment efficacy; and mortality.
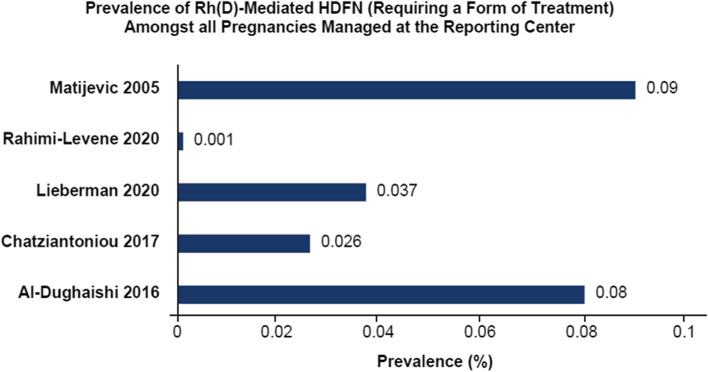
Results: We identified 2,541 articles. After excluding 2,482 articles and adding 1 article from screening systematic reviews, 60 articles were selected. Most abstracted data were from case reports and case series. Prevalence was 0.047% and 0.006% for Rh(D)- and K-mediated HDFN, respectively. Most commonly reported antenatal treatment was intrauterine transfusion (IUT; median frequency [interquartile range]: 13.0% [7.2-66.0]). Average gestational age at first IUT ranged between 25 and 27 weeks. weeks. This timing is early and carries risks, which were observed in outcomes associated with IUTs. The rate of hydrops fetalis among pregnancies with Rh(D)-mediated HDFN treated with IUT was 14.8% (range, 0-50%) and 39.2% in K-mediated HDFN. Overall mean ± SD fetal mortality rate that was found to be 19.8%±29.4% across 19 studies. Mean gestational age at birth ranged between 34 and 36 weeks.
Conclusion: These findings corroborate the rareness of HDFN and frequently needed intrauterine transfusion with inherent risks, and most births occur at a late preterm gestational age. We identified several evidence gaps providing opportunities for future studies.
Keywords: Fetal anemia; Fetal therapy; Hemolytic disease of the fetus and newborn; Intrauterine transfusion.
© 2023. The Author(s).
Conflict of interest statement
Derek P. de Winter: PhD program funded by Momenta Pharmaceuticals, Inc., which was acquired by Johnson & Johnson; coordinating investigator for a phase 2 trial (NCT03842189) of a new drug for the treatment of HDFN, which is sponsored by Janssen Pharmaceuticals.
Allysen Kaminski: Former employee of OPEN Health, which was retained by Janssen Pharmaceuticals to conduct the study.
May Lee Tjoa: Employee and stockholder of Janssen Pharmaceuticals.
Dick Oepkes: Former principal investigator for a phase 2 trial (NCT03842189) of a new drug for the treatment of HDFN, which is sponsored by Janssen Pharmaceuticals.
Figures
References
-
- Jackson ME, Baker JM. Hemolytic disease of the Fetus and Newborn: historical and current state. Clin Lab Med. 2021;41(1):133–51. - PubMed
-
- Raguz MJ, Prce Z, Bjelanovic V, Bjelanovic I, Dzida S, Mabic M. 20 years of follow-up alloimmunization and hemolytic disease in Newborn: has anything changed in the Field over the years? Klin Padiatr. 2020;232(6):314–20. - PubMed
-
- Legler TJ. RhIg for the prevention rh immunization and IVIg for the treatment of affected neonates. Transfus Apher Sci. 2020;59(5):102950. - PubMed
-
- Pollack W, Gorman JG, Freda VJ, Ascari WQ, Allen AE, Baker WJ. Results of clinical trials of RhoGAM in women. Transfusion. 1968;8(3):151–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
