

Relationships Between Social Vulnerability and Coronavirus Disease 2019 Vaccination Coverage and Vaccine Effectiveness
- PMID: 36611252
- PMCID: PMC10949185
- DOI: 10.1093/cid/ciad003
Relationships Between Social Vulnerability and Coronavirus Disease 2019 Vaccination Coverage and Vaccine Effectiveness
Abstract
Background: Coronavirus disease 2019 (COVID-19) vaccination coverage remains lower in communities with higher social vulnerability. Factors such as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) exposure risk and access to healthcare are often correlated with social vulnerability and may therefore contribute to a relationship between vulnerability and observed vaccine effectiveness (VE). Understanding whether these factors impact VE could contribute to our understanding of real-world VE.
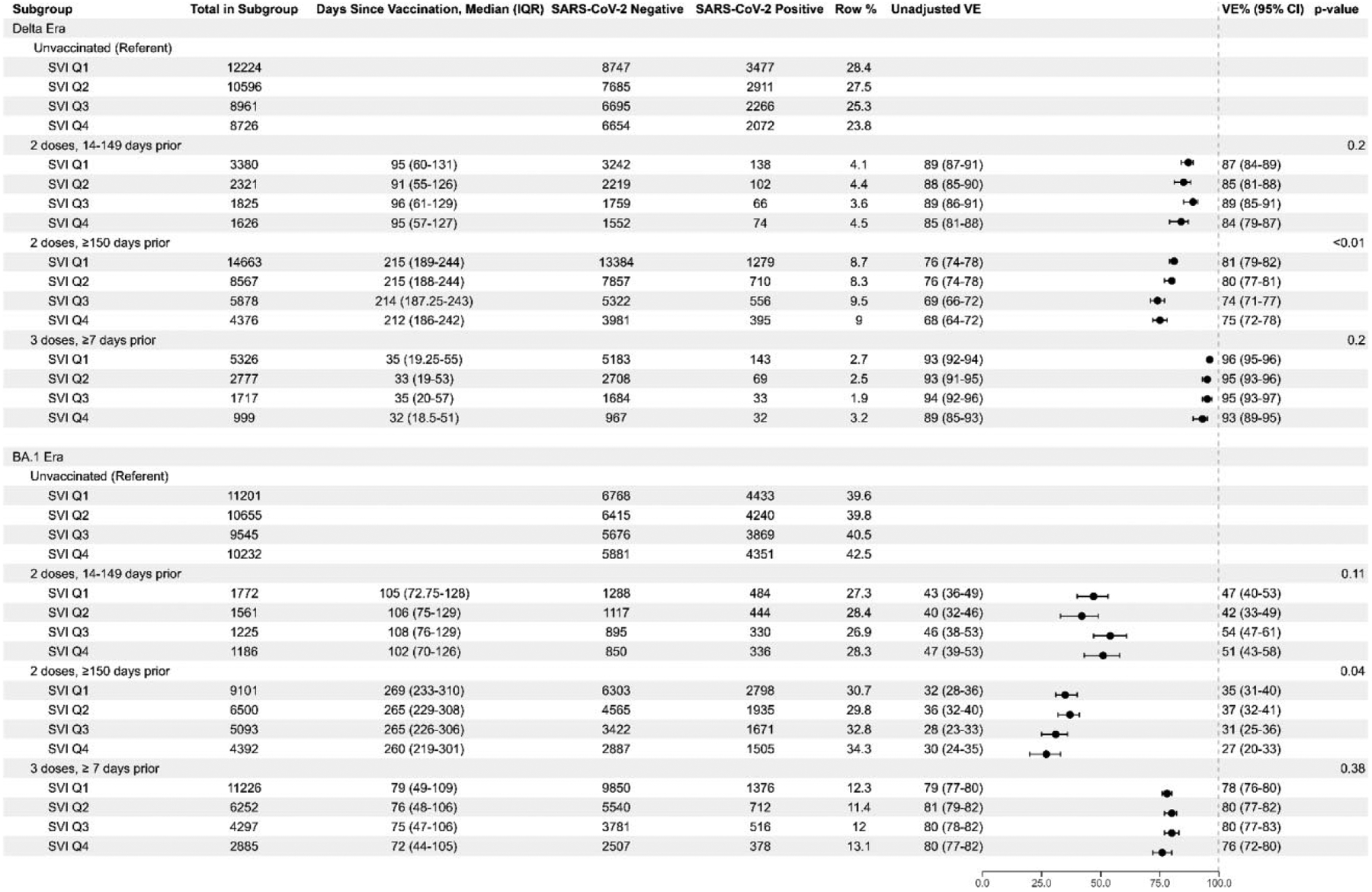
Methods: We used electronic health record data from 7 health systems to assess vaccination coverage among patients with medically attended COVID-19-like illness. We then used a test-negative design to assess VE for 2- and 3-dose messenger RNA (mRNA) adult (≥18 years) vaccine recipients across Social Vulnerability Index (SVI) quartiles. SVI rankings were determined by geocoding patient addresses to census tracts; rankings were grouped into quartiles for analysis.
Results: In July 2021, primary series vaccination coverage was higher in the least vulnerable quartile than in the most vulnerable quartile (56% vs 36%, respectively). In February 2022, booster dose coverage among persons who had completed a primary series was higher in the least vulnerable quartile than in the most vulnerable quartile (43% vs 30%). VE among 2-dose and 3-dose recipients during the Delta and Omicron BA.1 periods of predominance was similar across SVI quartiles.
Conclusions: COVID-19 vaccination coverage varied substantially by SVI. Differences in VE estimates by SVI were minimal across groups after adjusting for baseline patient factors. However, lower vaccination coverage among more socially vulnerable groups means that the burden of illness is still disproportionately borne by the most socially vulnerable populations.
Keywords: COVID-19; Social Vulnerability Index; vaccination coverage; vaccine effectiveness.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2023.
Conflict of interest statement
Potential conflicts of interest. B. E. D. reported consulting fees for advisory panel on HPV vaccination from Merck & Co and book royalties from Elsevier (book on HIE) as well as Springer Nature (book on Public Health Informatics), and grant to evaluate HIE technologies from US National Institutes of Health (NIH), grant to use HIE data for public health surveillance from CDC, R21 grant to evaluate HIE technologies from US Agency for Healthcare Research and Quality, grant to evaluate HIE technologies from US Department of Veterans Affairs. G. V. B. reported grants or contracts from Sanofi for Tdap Vaccine Safety and from CDC for Vaccine Safety Datalink. A. I. N. received institutional support from Pfizer for an unrelated study of meningococcal B vaccine safety during pregnancy and institutional research funding from Vir Biotechnology for unrelated influenza study. S. Rao received grant funding from GlaxoSmithKline. S. A. I. reports contract no. 200-2012-53584 (Vaccine Safety Datalink) from CDC. M. B. reports Columbia University is part of the VISION surveillance network and receives funding from Westat to support work done at Columbia as part of VISION. M. G. reports Ambulatory US Flu/COVID VE Network institutional grant, HAIVEN Adult Inpatient Flu/COVID VE institutional grant from CDC, IVY-3 PHS project institutional subcontract from CDC-Vanderbilt, and RECOVER study institutional subcontract from CDC-Abt. K. M. reports contracts or grants paid to institution from US CDC Ambulatory US Flu VE Network and US CDC HAIVEN—Hospitalized Adult Influenza Vaccine Effectiveness Network. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures



Comment in
-
The Last Mile Problem-Coronavirus Disease 2019 Vaccine Coverage Among the Most Socially Vulnerable.Clin Infect Dis. 2023 May 3;76(9):1626-1627. doi: 10.1093/cid/ciad006. Clin Infect Dis. 2023. PMID: 36611245 No abstract available.
References
-
- Centers for Disease Control and Prevention. COVID data tracker. Available at: https://covid.cdc.gov/covid-data-tracker. Accessed 4 August 2022.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
