

A Rare Case of a Primary Leiomyoma of the Clivus in an Immunocompetent Patient and a Review of the Literature Regarding Clival Lesions
- PMID: 36611301
- PMCID: PMC9818954
- DOI: 10.3390/diagnostics13010009
A Rare Case of a Primary Leiomyoma of the Clivus in an Immunocompetent Patient and a Review of the Literature Regarding Clival Lesions
Abstract
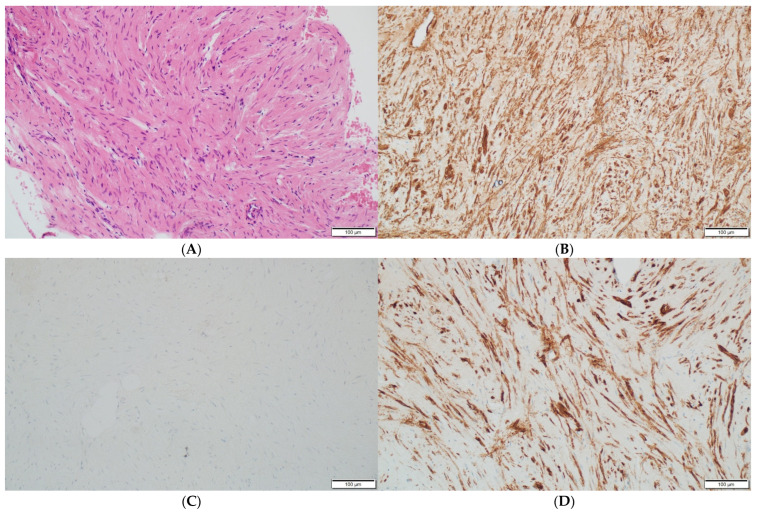
Leiomyomas are common lesions that are usually located in the genitourinary and gastrointestinal tracts. Primary leiomyomas at the skull base are uncommon. They are composed of well-differentiated smooth muscle cells without cellular atypia. The diagnosis of a leiomyoma has to be confirmed by immunohistochemistry. The tumor tissue is immunoreactive for SMA, S100 and cytokeratin. Leiomyomas mainly occur in immunocompromised patients. Most tumor tissues are positive for EBV. The presented case is that of a 56-year-old immunocompetent woman with a tumor on the clivus. The radiological images suggested chordoma or fibrous dysplasia. Transnasal transsphenoidal surgery was performed. The tumor tissue consisted of well-differentiated smooth muscle cells with elongated nuclei. Immunohistochemistry revealed a positive reaction for desmin, SMA and h-Caldesmon and a negative reaction for S100, beta-catenin, PGR and Ki67. The leiomyoma diagnosis was subsequently established. To the best of our knowledge, the case of a primary leiomyoma on the clivus of an immunocompetent patient is the first to be described. We also extensively reviewed the literature on the immunohistopathological and radiological differential diagnosis of clival lesions.
Keywords: chordoma; clival diseases; clivus; fibrous dysplasia; primary leiomyoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Cutaneous Leiomyoma Mimicking a Keloid.Acta Dermatovenerol Croat. 2020 Aug;28(2):116. Acta Dermatovenerol Croat. 2020. PMID: 32876039
-
Fungal skull base lesion masquerading as malignancy: a diagnostic dilemma. Illustrative case report.Ann Med Surg (Lond). 2024 Dec 20;87(2):929-933. doi: 10.1097/MS9.0000000000002964. eCollection 2025 Feb. Ann Med Surg (Lond). 2024. PMID: 40110306 Free PMC article.
-
Fibrous dysplasia of the clivus.J Korean Neurosurg Soc. 2010 Nov;48(5):441-4. doi: 10.3340/jkns.2010.48.5.441. Epub 2010 Nov 30. J Korean Neurosurg Soc. 2010. PMID: 21286483 Free PMC article.
-
Fibrous dysplasia of the clivus with a second T8 bone lesion: case report.Surg Neurol. 2006 Feb;65(2):202-5; discussion 205-6. doi: 10.1016/j.surneu.2005.05.025. Surg Neurol. 2006. PMID: 16427429 Review.
-
Primary iris leiomyoma.Surv Ophthalmol. 2017 May-Jun;62(3):366-370. doi: 10.1016/j.survophthal.2016.11.007. Epub 2016 Nov 24. Surv Ophthalmol. 2017. PMID: 27890619 Review.
Cited by
-
Case report: Successful bronchoscopic interventional treatment of endobronchial leiomyomas.Open Life Sci. 2024 May 7;19(1):20220845. doi: 10.1515/biol-2022-0845. eCollection 2024. Open Life Sci. 2024. PMID: 38737105 Free PMC article.
References
-
- Davis J.L., Tihan T., Kilpatrick S.E. 14-Mesenchymal Tumors of the Central Nervous System. In: Perry A., Brat D.J., editors. Practical Surgical Neuropathology: A Diagnostic Approach. 2nd ed. Elsevier; Amsterdam, The Netherlands: 2018. pp. 299–322. - DOI
-
- Colagrande A., Cazzato G., Fedele S., Andriola V., Ingravallo G., Resta L., Vincenti L. A Unique Case of the Transformation of a Hepatic Leiomyoma into Leiomyosarcoma with Pancreatic Metastases: Review of the Literature with Case Presentation. Reports. 2022;5:2. doi: 10.3390/reports5010002. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
