

Ischiofemoral Impingement Syndrome: Clinical and Imaging/Guidance Issues with Special Focus on Ultrasonography
- PMID: 36611431
- PMCID: PMC9818255
- DOI: 10.3390/diagnostics13010139
Ischiofemoral Impingement Syndrome: Clinical and Imaging/Guidance Issues with Special Focus on Ultrasonography
Abstract
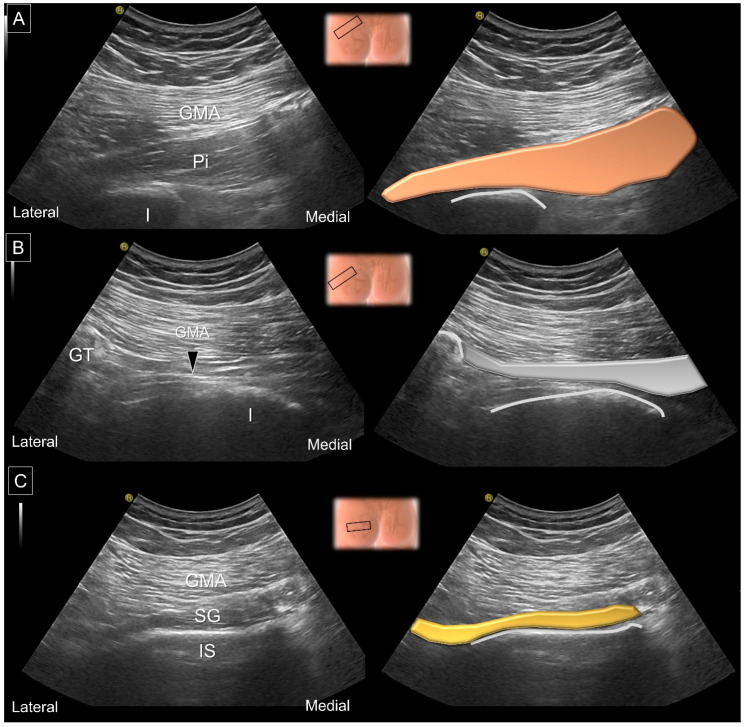
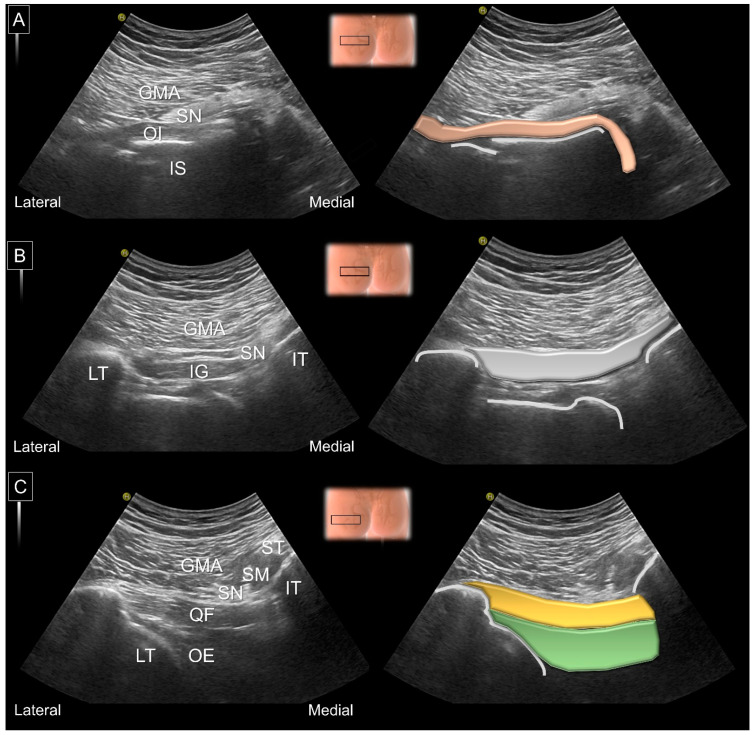
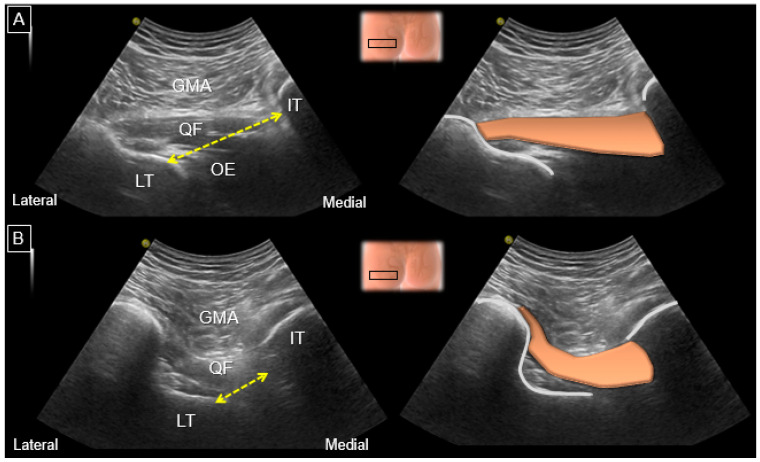
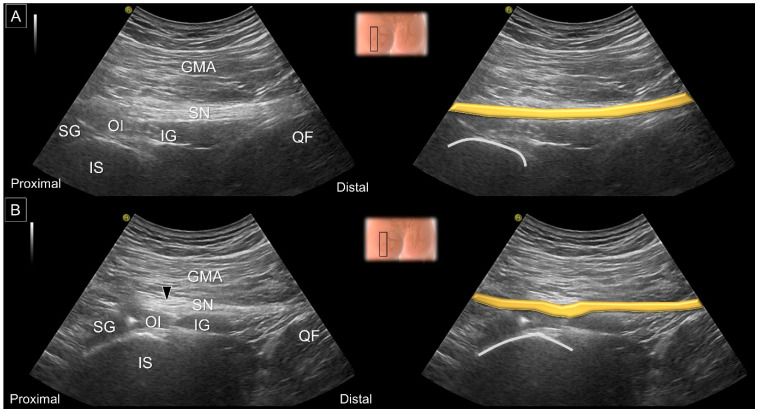
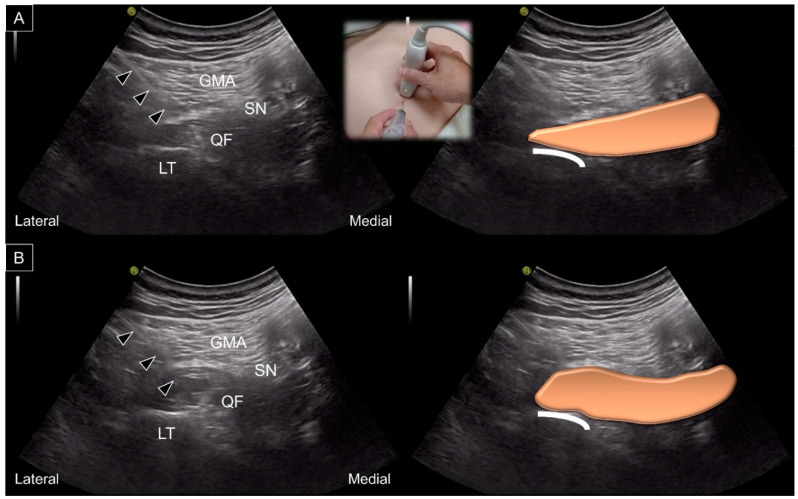
Ischiofemoral impingement syndrome is a neglected cause of posterior hip pain which is derived from narrowing of the space between the lateral aspect of the ischium and the medial aspect of the lesser trochanter. Its diagnosis is challenging and requires the combination of physical tests and imaging studies. In the present narrative review, we found that femoral anteversion predisposes patients to the narrowing of the ischiofemoral space and subsequent quadratus femoris muscle injury. Magnetic resonance imaging serves as the gold-standard diagnostic tool, which facilities the quantification of the ischiofemoral distance and the recognition of edema/fat infiltration/tearing of the quadratus femoris muscle. Ultrasound is useful for scrutinizing the integrity of deep gluteal muscles, and its capability to measure the ischiofemoral space is comparable to that of magnetic resonance. Various injection regimens can be applied to treat ischiofemoral impingement syndrome under ultrasound guidance and they appear to be safe and effective. Finally, more randomized controlled trials are needed to build solid bases of evidence on ultrasound-guided interventions in the management of ischiofemoral impingement syndrome.
Keywords: hip pain; ischiofemoral impingement; magnetic resonance imaging; quadratus femoris; ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Sundén-Lundius A., Johnsson B., Lohmander S., Ekdahl C. Prevalence of self-reported hip disorders, relations to age, gender, pain, stiffness, weakness and other joint disorders. Adv. Physiother. 2005;7:108–113. doi: 10.1080/14038190510010395. - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
