

Clinicopathological and Dermoscopic Baselines in Patients with Lynch Syndrome
- PMID: 36612110
- PMCID: PMC9817705
- DOI: 10.3390/cancers15010114
Clinicopathological and Dermoscopic Baselines in Patients with Lynch Syndrome
Abstract
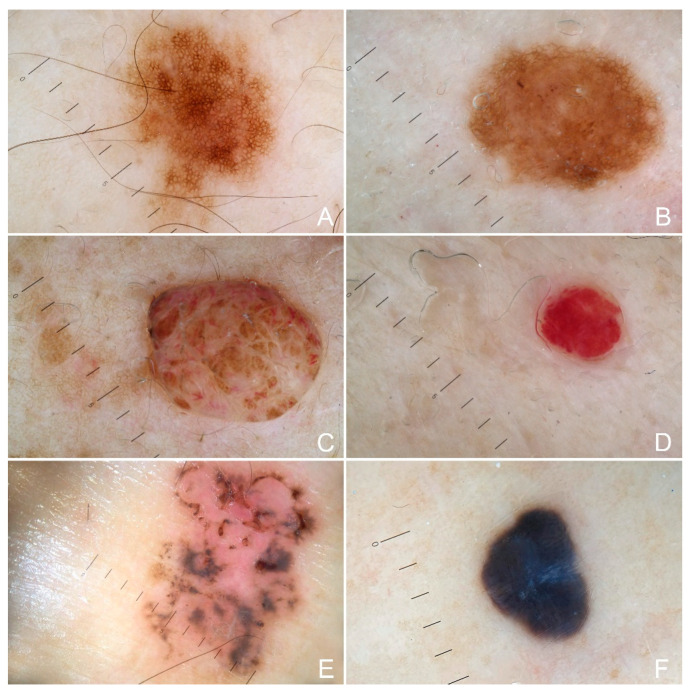
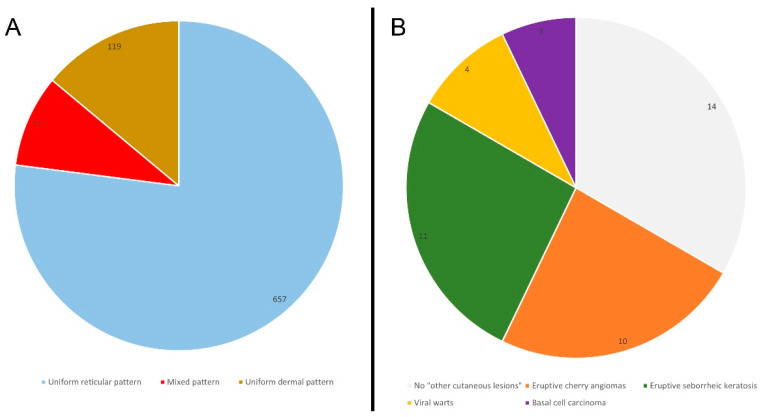
Despite the fact that Lynch Syndrome (LS) patients may also develop extra-colonic malignancies, research evaluating the association between LS and skin cancers is currently very limited. We performed a monocentric clinical and dermoscopic study involving 42 LS patients which referred to the Dermatology Unit for cutaneous screenings. In total, 22 patients showed a mutation in MLH1 and 17 patients a MSH2 mutation. Out of the entire cohort, 83% of LS patients showed brown hairs and 78% brown eyes, and the most frequent phototypes were III and II (respectively, 71.5% and 21%). A positive medical history for an internal malignancy was present in 36% of patients, with colon cancer as the most frequent malignancy in 60% of cases. A total of 853 cutaneous lesions have been analyzed: 47% of patients showed a total number of nevi > 10. The main observed dermoscopic features were a uniform reticular pattern (77% of patients), a mixed pattern (9% of patients) and a uniform dermal pattern (14% of patients). Eruptive cherry angiomas were present in 24% of cases, eruptive seborrheic keratosis in 26% and viral warts in 7% of cases; basal cell carcinoma was detected in 7% of cases. We have not found specific associations with specific skin manifestations, and the clinical and dermoscopic appearance of the pigmented lesions reflected the features present in the general population. To date, there are currently no guidelines for skin screening in LS patients. According to our study, there is insufficient evidence to ensure increased surveillance in LS patients; further studies with larger samples of patients are needed to better investigate dermatological and dermoscopic features in LS carriers.
Keywords: Lynch syndrome; MMR; cutaneous lesions; dermoscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Dermatological and Dermoscopic Baselines in BRCA Mutation Carriers.Front Med (Lausanne). 2022 Apr 29;9:863468. doi: 10.3389/fmed.2022.863468. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35573021 Free PMC article.
-
A comparison of dermoscopic features among lentigo senilis/initial seborrheic keratosis, seborrheic keratosis, lentigo maligna and lentigo maligna melanoma on the face.J Dermatol. 2004 Nov;31(11):884-9. doi: 10.1111/j.1346-8138.2004.tb00621.x. J Dermatol. 2004. PMID: 15729860
-
Dermoscopic Features of Giant Molluscum Contagiosum in a Patient with Acquired Immunodeficiency Syndrome.Acta Dermatovenerol Croat. 2020 Dec;28(7):233-235. Acta Dermatovenerol Croat. 2020. PMID: 33834996
-
Genitourinary manifestations of Lynch syndrome in the urological practice.Asian J Urol. 2022 Oct;9(4):443-450. doi: 10.1016/j.ajur.2022.05.009. Epub 2022 Aug 31. Asian J Urol. 2022. PMID: 36381590 Free PMC article. Review.
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
Cited by
-
Skin Signals: Exploring the Intersection of Cancer Predisposition Syndromes and Dermatological Manifestations.Int J Mol Sci. 2025 Jun 26;26(13):6140. doi: 10.3390/ijms26136140. Int J Mol Sci. 2025. PMID: 40649916 Free PMC article. Review.
References
-
- da Silva F.C., de Oliveira L.P., Santos E.M., Nakagawa W.T., Aguiar Junior S., Valentin M.D., Rossi B.M., de Oliveira Ferreira F. Frequency of extracolonic tumors in Brazilian families with Lynch syndrome: Analysis of a hereditary colorectal cancer institutional registry. Fam. Cancer. 2010;9:563–570. doi: 10.1007/s10689-010-9373-2. - DOI - PubMed
-
- Møller P., Seppälä T., Bernstein I., Holinski-Feder E., Sala P., Evans D.G., Lindblom A., Macrae F., Blanco I., Sijmons R., et al. Cancer incidence and survival in Lynch syndrome patients receiving colonoscopic and gynaecological surveillance: First report from the prospective Lynch syndrome database. Gut. 2017;66:464–472. doi: 10.1136/gutjnl-2015-309675. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
