

Present and Future Role of Immune Targets in Acute Myeloid Leukemia
- PMID: 36612249
- PMCID: PMC9818182
- DOI: 10.3390/cancers15010253
Present and Future Role of Immune Targets in Acute Myeloid Leukemia
Abstract
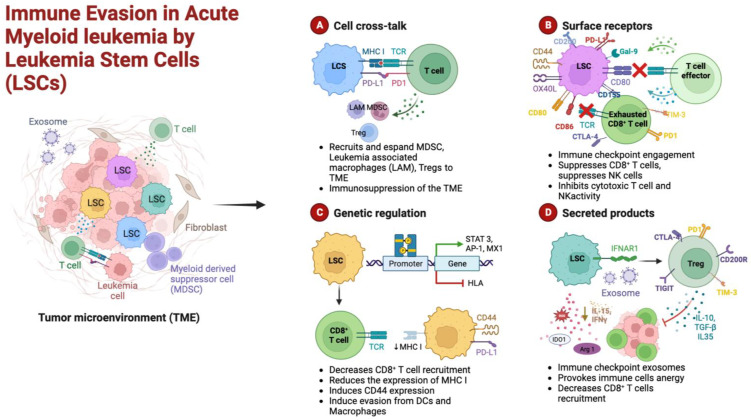
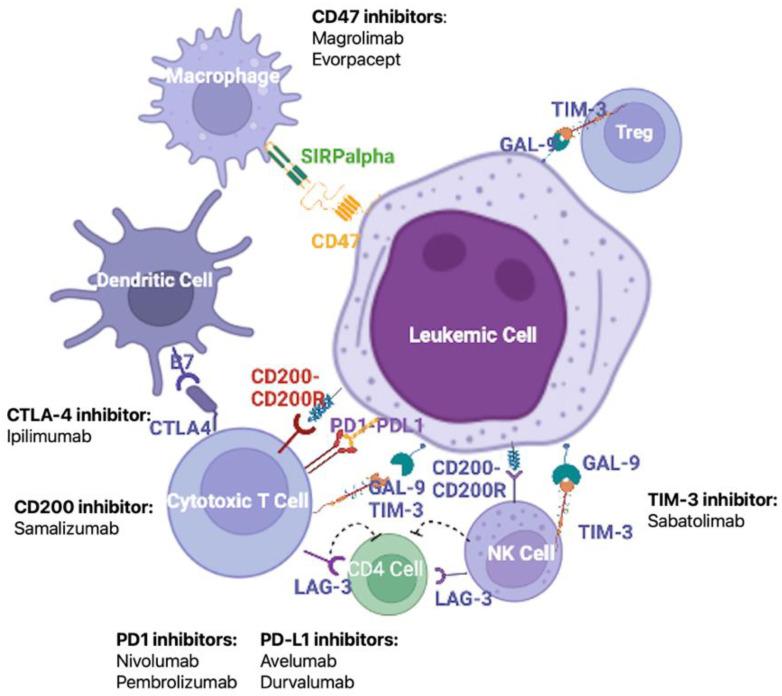
It is now well known that the bone marrow (BM) cell niche contributes to leukemogenesis, but emerging data support the role of the complex crosstalk between AML cells and the BM microenvironment to induce a permissive immune setting that protects leukemic stem cells (LSCs) from therapy-induced death, thus favoring disease persistence and eventual relapse. The identification of potential immune targets on AML cells and the modulation of the BM environment could lead to enhanced anti-leukemic effects of drugs, immune system reactivation, and the restoration of AML surveillance. Potential targets and effectors of this immune-based therapy could be monoclonal antibodies directed against LSC antigens such as CD33, CD123, and CLL-1 (either as direct targets or via several bispecific T-cell engagers), immune checkpoint inhibitors acting on different co-inhibitory axes (alone or in combination with conventional AML drugs), and novel cellular therapies such as chimeric antigen receptor (CAR) T-cells designed against AML-specific antigens. Though dozens of clinical trials, mostly in phases I and II, are ongoing worldwide, results have still been negatively affected by difficulties in the identification of the optimal targets on LSCs.
Keywords: acute myeloid leukemia; drug resistance; immune escape; immune therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Khoury J.D., Solary E., Abla O., Akkari Y., Alaggio R., Apperley J.F., Bejar R., Berti E., Busque L., Chan J.K.C., et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia. 2022;36:1703–1719. doi: 10.1038/s41375-022-01613-1. - DOI - PMC - PubMed
-
- Dohner H., Wei A.H., Appelbaum F.R., Craddock C., DiNardo C.D., Dombret H., Ebert B.L., Fenaux P., Godley L.A., Hasserjian R.P., et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140:1345–1377. doi: 10.1182/blood.2022016867. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
