

Bentall Operation: Early Surgical Results, Seven-Year Outcomes, and Risk Factors Analysis
- PMID: 36612535
- PMCID: PMC9820033
- DOI: 10.3390/ijerph20010212
Bentall Operation: Early Surgical Results, Seven-Year Outcomes, and Risk Factors Analysis
Abstract
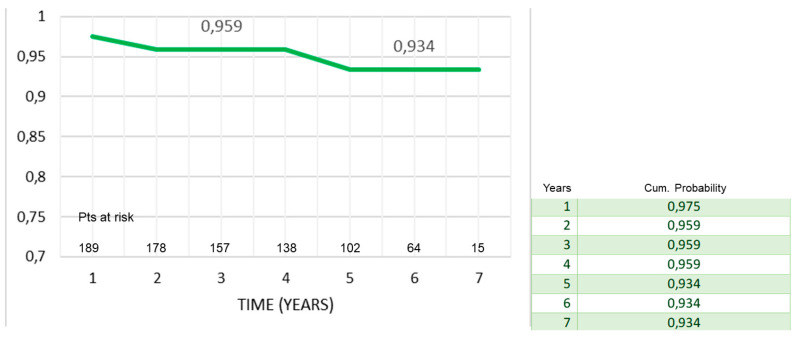
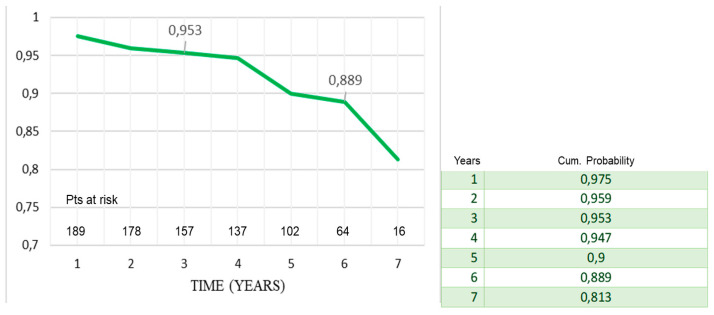
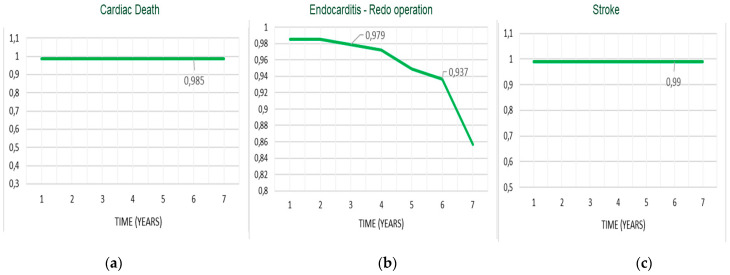
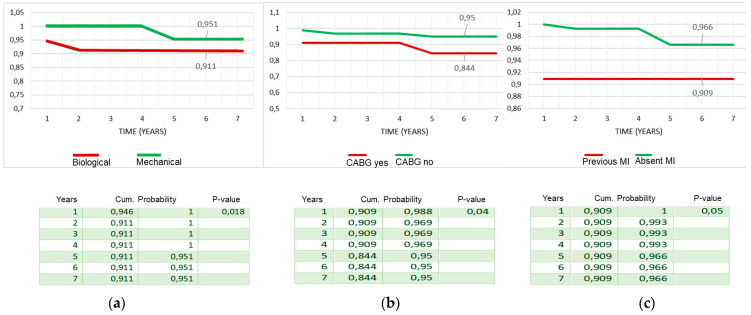
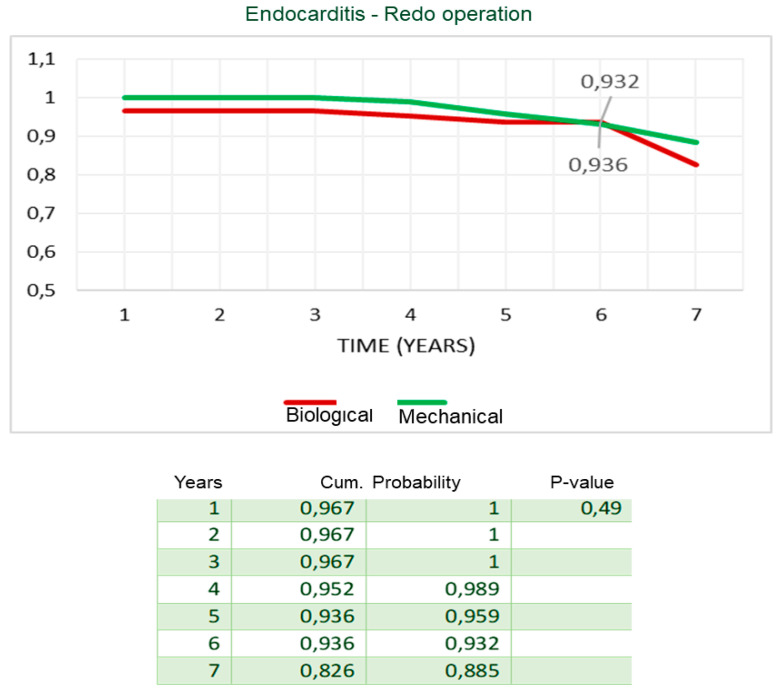
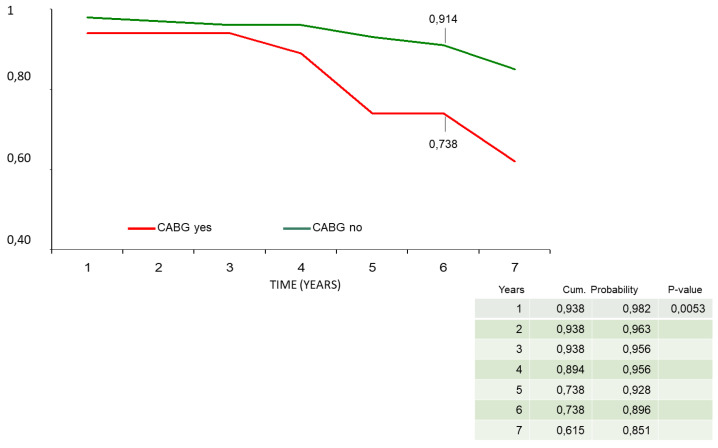
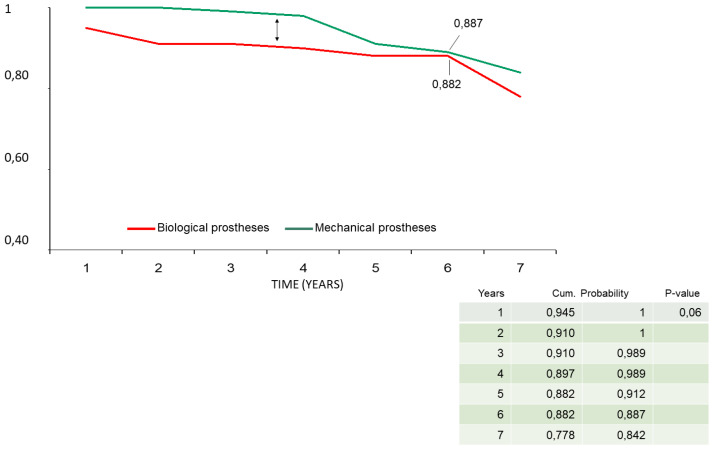
Aim: To analyze early and mid-term outcomes of the Bentall operation. Methods: Two hundred and seventeen patients (mean age 65.6 ± 15.9 years, males/females 172/45) underwent Bentall operation in a 7-year period (January 2015−December 2021), on average, 30 Bentall operations occurred per year, using biological (n = 104) or mechanical (n = 113) valved conduits for the treatment of ascending aorta−aortic root aneurysms. Associate procedures were performed in 58 patients (26.7%); coronary artery bypass grafting (CABG) in 35 (16%). Mean follow-up was 55.2 ± 24 (median 60.2) months. Cox model analysis was used to assess risk factors, Kaplan−Meier and log-rank tests were used to assess different survival rates. Results: Operative mortality was 1.38%. At 7 years, survival, freedom from cardiac death, and event-free survival were 93% ± 2%, 99% ± 1%, and 81% ± 5%. NYHA class (p < 0.0001), trans-aortic valve mean (p < 0.0001) and maximum (p < 0.000) gradients, left ventricular hypertrophy (p < 0.05), and pulmonary arterial pressure (p = 0.002) significantly improved vs. preoperative values. Concomitant CABG during Bentall operation independently affected late outcomes (HR 1.9−2.3; p-values < 0.05). Late survival was affected by concomitant CABG (84% ± 8% vs. 95% ± 2%, p = 0.04), preoperative myocardial infarction (91% ± 9% vs. 97% ± 2%, p = 0.02), and biological vs. mechanical prostheses valved conduits (91% ± 9% vs. 95% ± 3%, p = 0.02). Event-free survival also was affected by concomitant CABG (62% ± 14% vs. 85% ± 5%, p = 0.005) and biological prostheses (78% ± 8% vs. 84% ± 6%, p = 0.06). Freedom from endocarditis−redo operation was 83% ± 9% for biological prostheses vs. 89% ± 6% for mechanical prostheses (p = 0.49). Conclusions: Low rates of operative mortality and late complications make Bentall operation the gold standard for the treatment of ascending aorta−aortic root aneurysms. Coronary ischemic disease affects late outcomes. Biological prostheses should be preferred for the elderly.
Keywords: Bentall operation; aortic root surgery; ascending aorta replacement.
Conflict of interest statement
All the authors declare that they have no competing financial interests or personal relationships that could have influenced the work reported in this paper.
Figures
References
-
- Wallen T., Habertheuer A., Bavaria J.E., Hughes G., Badhwar V., Jacobs J.P., Yerokun B., Thibault D., Milewski K., Desai N., et al. Elective Aortic Root Replacement in North America: Analysis of STS Adult Cardiac Surgery Database. Ann. Thorac. Surg. 2019;107:1307–1312. doi: 10.1016/j.athoracsur.2018.12.039. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
